Overview of Michigan Certificate-of-Need laws
Certificate-of-need laws vary from state to state but generally require health care providers to get government permission before adding or expanding facilities and services. In turn, existing health care facilities maintain government-approved monopolies on health care services by restricting supply, which limits patient access and suppresses innovation. Because they block competition, CON laws, not surprisingly, are associated with higher health care costs and fewer medical services per capita.
Michigan’s CON commission includes representatives from existing health care providers, putting doctors and nurses in the position of seeking permission from their competitors before beginning or expanding practice. Obstructing health care expansion reduces the number of available hospital beds, restricts vital diagnostic services in hospitals, and prevents medical professionals from meeting the needs of Michiganders.
The federal government initially championed CON laws, and the 1974 National Health Planning and Resources Development Act encouraged states to pass such laws or risk losing federal health planning resources. The hope was that CON laws would restrain health care spending, increase quality and improve access.
Congress repealed the act in 1986, after CON laws failed to achieve their stated goals. Since then, a dozen states, representing roughly 40% of the American people, have fully repealed their CON laws. But 38 states and the District of Columbia maintain CON laws or similar restrictions.
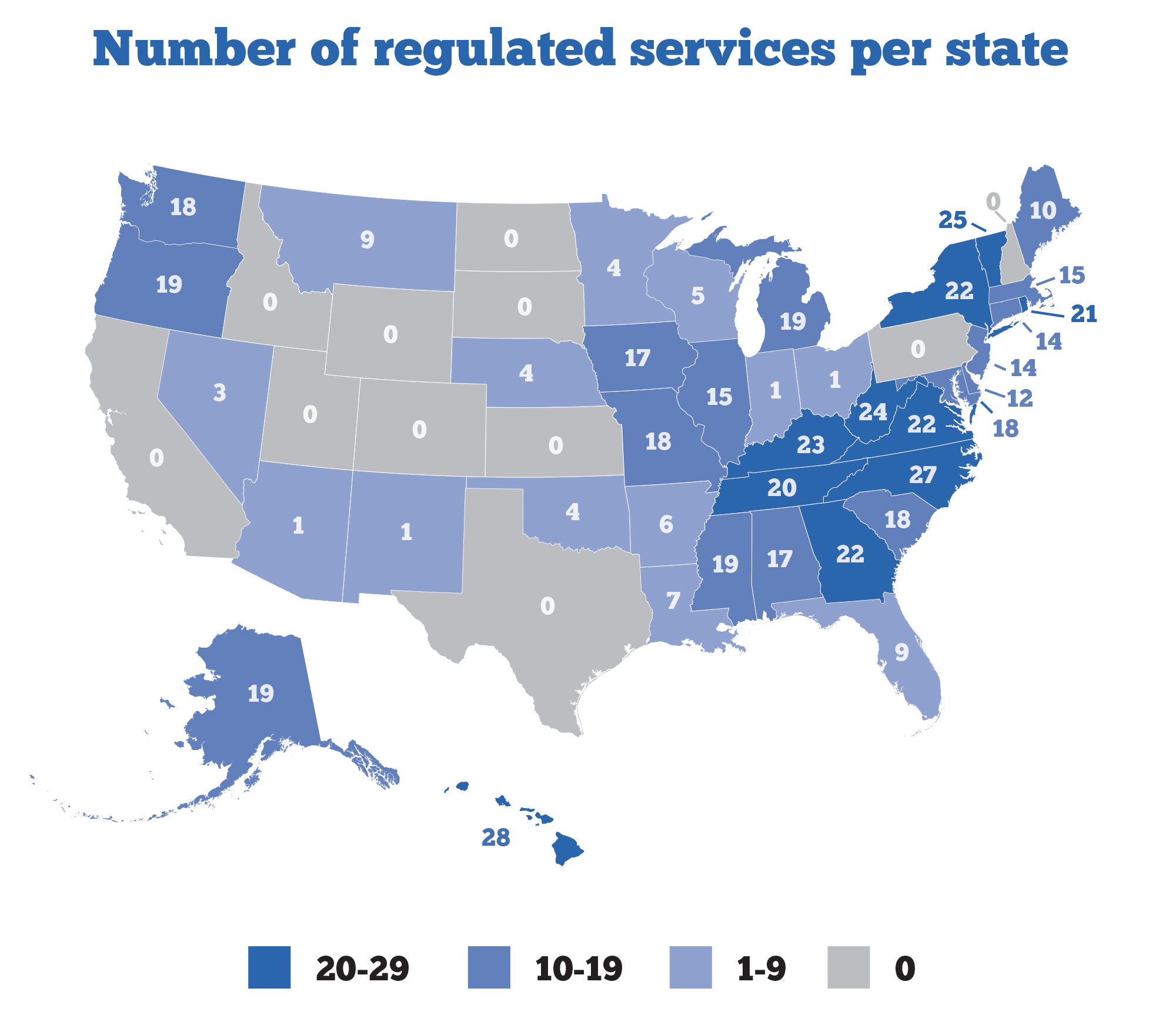
There is no uniformity to the way that states with CON laws use them. Some states have just one regulated system, but others have upwards of 40. Some laws apply only in urban areas and exempt rural areas. The fact that these laws vary from state to state — some have no laws while others have dozens — indicates that they are less about public safety and controlling costs and more about restricting much-needed competitive forces.
A national review of 39 CON jurisdictions found no “rhyme or reason to what services require a CON.” This finding, it concluded, “strongly suggests that CONs are driven less by the government’s perception of what will improve patient health and more by lobbying efforts of powerful insider groups within each state.”
Decades of research has found that CON laws reduce access to care, decrease health care quality and increase costs. Left- and right-leaning groups, the American Medical Association, the Federal Trade Commission and the Department of Justice recognize the harmful effects of CON laws and have called for their elimination. Thus far, 12 states have completely repealed their CON laws, three states administer limited versions, and another two dozen or so have fewer CON regulations than Michigan.
As recently as 2015, the Federal Trade Commission and the antitrust division of the U.S. Department of Justice wrote in a joint statement that “CON laws can prevent the efficient functioning of health care markets in several ways that may undermine” the “goals of reducing health care costs and improving access to care.” The FTC has advocated against CON laws for decades “because they prevent health care providers from responding quickly to meet market demand.”
The COVID-19 pandemic highlighted the problem of CON laws. That’s why early on, at least 25 jurisdictions, including Michigan, suspended or loosened their CON requirements to meet changing market demands and medical needs. As a result of those actions, patients – both COVID and non-COVID – benefited. Research from the Mercatus Center at George Mason University found that “states without CON laws between mid-March and late June 2020 had fewer hospital deaths than states with CON laws and that more than half of these lives saved were non-COVID patients.”
In Michigan, an 11-person CON commission oversees the CON review standards, which are used to approve or deny various CON applications. The members, who are subject to Senate confirmation, develop, approve, disapprove or revise the standards. By law, the members must be representatives of existing hospitals, health care professionals, employers (some self-insured, others, not) and labor unions. This makeup creates an ongoing conflict of interest between existing providers and new ones who must get approval from their competitors before adding additional bed capacity, technologies, facilities, and emergency transportation services. No one on the commission represents consumers. As a result, consumer needs sometimes go unmet.
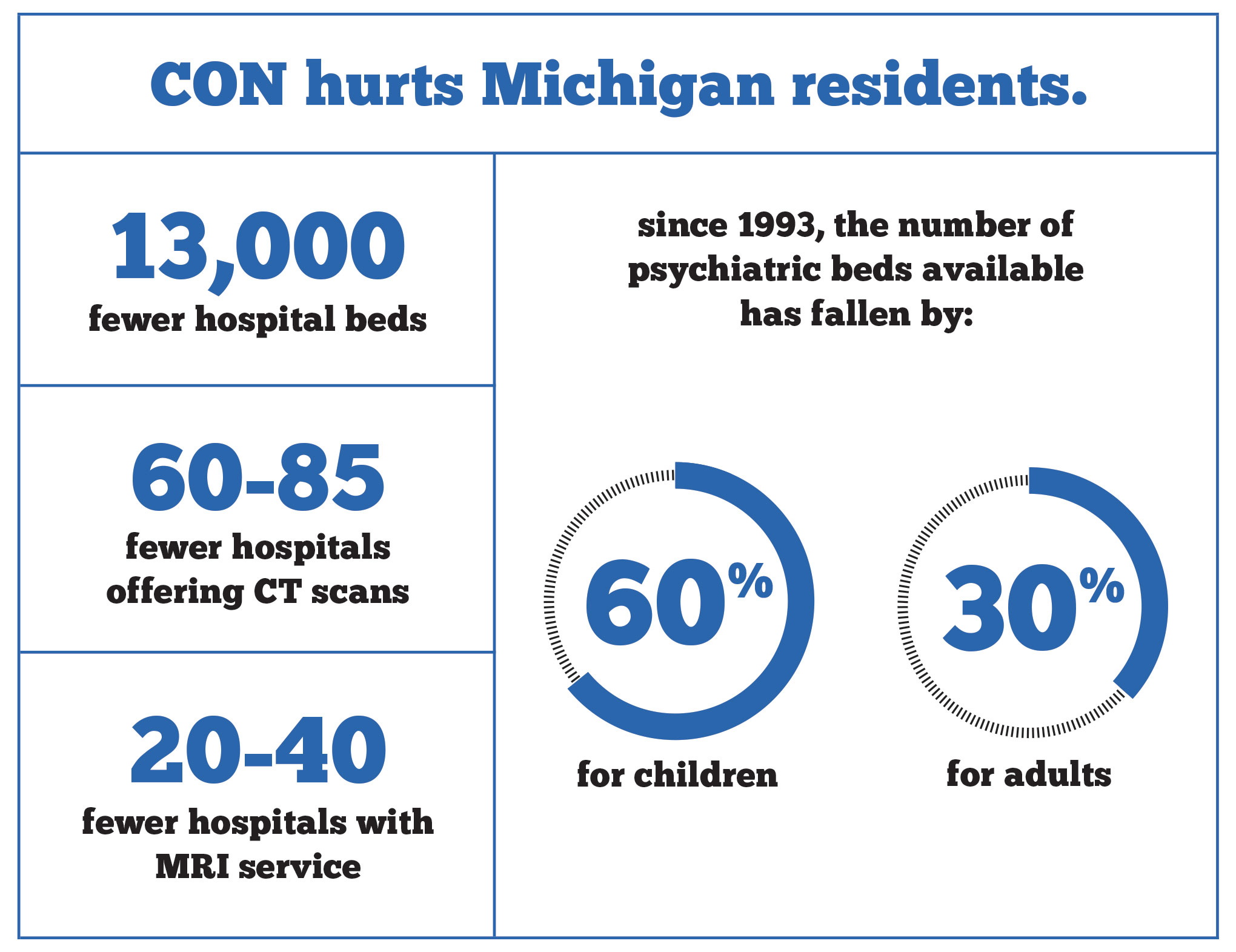
Despite a need for more psychiatric beds, for example, a proposed 60-bed expansion for adult in-patient psychiatric beds at Pine Rest Christian Mental Health Services was denied in April 2021. According to a 2018 workgroup report from the Michigan Department of Health and Human Services, the total number of community-based inpatient psychiatric beds has fallen by nearly 30% for adults and over 60% for children since 1993. Patients with mental illnesses may not receive care when they need it and have to wait longer in emergency rooms or, in some cases, even jail cells.
Michigan currently requires 25 different certificates of need, including for hospitals and hospital beds, psychiatric hospitals and psychiatric beds, nursing homes and nursing home beds, and medical imaging services such as CT, MRI, and PET scans.
The threat of additional CON regulations persists. The CON Commission proposed regulations to limit the number of hospitals that could perform a cancer treatment therapy known as CAR T-cell cancer treatment, which uses a patient’s immune cells to fight cancer. The Michigan Legislature rejected these new regulations in October 2019.
What’s the impact of these CON laws on Michigan specifically? Research shows that Michigan CON laws result in nearly 13,000 fewer hospital beds, between 20 and 40 fewer hospitals offering MRI services, and between 60 and 85 fewer hospitals offering computed tomography (CT) scans.
Recommendation: Require more transparency, phase out, and fully repeal CON laws and regulations
Ultimately, Michigan should work to fully repeal all its CON laws. Given the entrenched interests in doing so, this might be difficult to do outright.
There are other options for reforming Michigan’s CON laws. Michigan could consider partially repealing regulations on certain services or technologies, or phase them out over time with automatic sunsets. Rejecting new regulations, like those proposed on CAR T-cell cancer treatments, is also key.
As patients continue to return to in-person care and treatments and vaccines are approved to curtail the spread of COVID-19, health care professionals and health facilities will need to respond to patient demand. Michigan CON laws stand in the way of providing the necessary beds and services.
Overview of Michigan scope-of-practice laws
Scope-of-practice restrictions prohibit health care providers from practicing to the full extent of their training. More specifically, scope-of-practice laws are regulations that restrict what tasks physician assistants (PAs), nurse practitioners (NPs), nurses, pharmacists, and other essential health care providers may perform while caring for their patients, regardless of their training, education, or experience. Scope-of-practice restrictions reduce the number of primary care givers available, and fewer choices for patients and consumers mean higher costs, longer wait times, and difficulty in getting treated. This is especially noticeable in rural areas of Michigan as well as during times public health emergencies.
Scope-of-practice laws essentially come down to how much autonomy a health care professional has when treating patients. For example, states have enacted a variety of rules covering nurse practitioners and physician assistants. One type restricts the ability of these professionals to prescribe mediations, including which kinds. Another is whether a nurse practitioner or a physician assistant is required to work under the supervision of a physician.
Opponents of reform argue that these laws are a safety issue for patients, but the evidence suggests otherwise. One study compared outcomes for patients receiving primary care follow-up and ongoing care after emergency department or urgent care visits. Patients were randomly assigned to a nurse practitioner or a physician, but the study found comparable outcomes, with no significant differences in patients’ health status.
In fact, the subjective evaluation of patients revealed a preference for NPs. “Patients were more satisfied with consultations with nurse practitioners than those with doctors.”
Several areas of Michigan have a shortage of primary care physicians. This may be caused by an overall shortage of primary care physicians, or an uneven displacement of them. Regardless of the reason, vulnerable populations — those on Medicaid, the poor and uninsured, Michiganders with disabilities, and those living in rural areas — have less access to primary care providers. Research shows that nurse practitioners are significantly more likely than primary care physicians to care for these vulnerable populations. NPs also accept lower payments, making care more affordable and more accessible.
Pharmacists are another underused health care provider capable of performing more within their scope of practice. They are also the providers that most Michiganders have easier access to, even in shortage areas. Patients find them in community pharmacies, physicians’ offices, hospitals, long-term care facilities, community health centers, managed care organizations, hospice settings, and the uniformed services. Nearly 90% of Americans live within five miles of a community pharmacy, giving these health care providers an opportunity to better integrate themselves into patients’ health care. Also, pharmacists have the most knowledge of medication therapy of any health professional.
Restrictions on Michigan’s primary care professionals
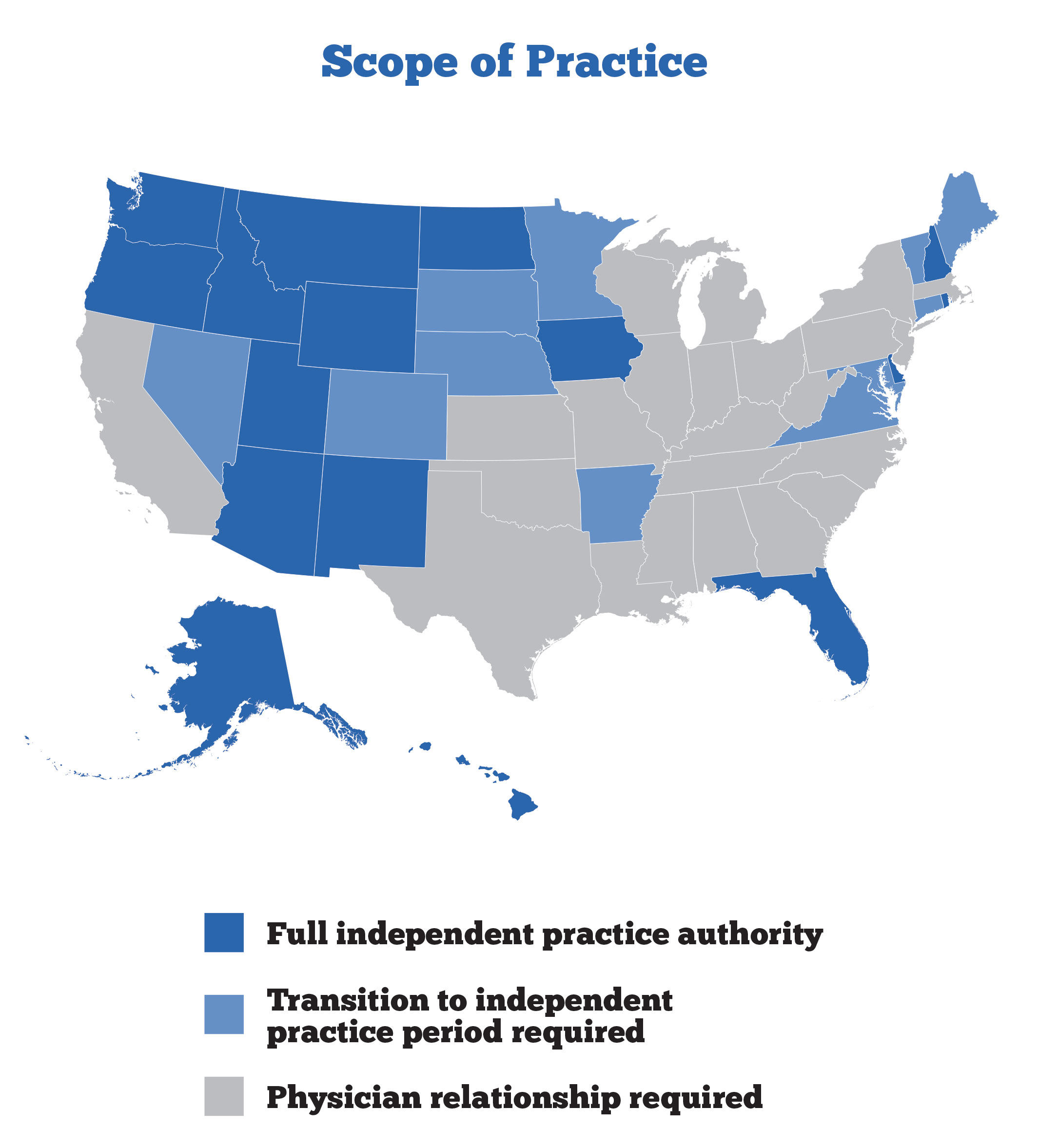
Michigan law allows for nurse practitioners but restricts them from practicing without the supervision of a physician, even though many of these professionals are educated at the doctoral level and have many years of clinical experience. Instead, these advanced practicing nurses must have a formal agreement with a supervising physician to practice. They must be delegated tasks and functions by a physician. Nurse practitioners are also not explicitly recognized in state policy as primary care providers.
While all states impose some form of scope-of-practice restrictions on medical professions, the specifics vary widely. According to Deena Kelly Costa, an assistant professor at the University of Michigan School of Nursing, Michigan has some of the nation’s most restrictive scope-of-practice laws for advanced practice nurses. Costa advised Gov. Gretchen Whitmer’s office in crafting the executive order suspending scope-of-practice restrictions. Costa highlighted research by the RAND Corporation that found eliminating these regulations for nurse practitioners would increase public access to health care.
Nurse practitioners are not the only medical professionals who must be supervised by a doctor. Michigan pharmacists have been able to administer vaccines to patients since 1995, but only as a delegated task under a collaborative practice agreement with a physician.
Recommendation: Allow nurse practitioners to provide patient care without immediate physician supervision to the extent of their training and capacities; expand current state pharmacists’ immunization authority to take advantage of their accessibility and training
In times of a public health emergency, scope-of-practice restrictions have a negative impact on health care delivery, especially as health professionals get sick while caring for patients, while hospital and clinic capacities are pushed to their limits. That’s why we saw several emergency scope-of-practice laws suspended in states across the country, including here in Michigan.
One of Gov. Whitmer’s emergency executive orders allowed physician assistants and nurse practitioners to provide care within their scope of practice without a written practice agreement or the supervision of a physician. The governor acknowledged that “suspending these scope of practice laws saved countless lives and ensured our hospitals were fully staffed to care for COVID-19 patients,” which is why Michigan policymakers should make this reform permanent. Additionally, they should allow PAs and NPs to operate autonomous practices without agreements with physicians, which would expand access to high-quality primary care and reduce costs.
The availability and accessibility of pharmacists provides an immediate opportunity to expand certain aspects of primary care. Policymakers should allow pharmacists to practice at the top of their education and training. In general, a pharmacist is taught how to recognize and dispense medications to treat a patient with chronic diseases, like diabetes, high blood pressure or heart disease. But to do this, pharmacists are required to have a collaborative practice agreement with a physician. For a period during the COVID-19 emergency, this scope-of-practice restriction was temporarily suspended. According to an executive order, the suspension would allow pharmacists to “provide care for routine health maintenance, chronic disease states, or similar conditions,” without a collaborative practice agreement, as long as they had been trained properly.
Many rural pharmacists are not able to obtain collaborative practice agreements due to the time, effort, and cost to maintain the service. Others simply can’t find a physician to collaborate with. Allowing pharmacists to test, treat, and prescribe medication for common illnesses like the flu and strep without these agreements would help reduce costs and improve health outcomes. This is especially valuable for vulnerable groups who have limited access to health professionals. Additionally, increasing a pharmacist’s authority to administer vaccines would improve access to immunizations and decrease health care gaps. Pharmacists should be allowed to offer any vaccine that is approved by the Centers for Disease Control and Prevention, Advisory Committee on Immunization Practices and the Federal Drug Administration, including vaccines that are under emergency use authorization.
In summary, restrictions on various health professionals can strain the health care system and slow its response during public health emergencies. Suspending scope-of-practice restrictions and supervisory requirements would help free up providers to do more.
Overview of Michigan telemedicine laws
Telemedicine is the use of communication technologies, like phones, tablets, or computers, to connect a patient with a health care professional in a different location. Telemedicine is viewed as both a cost-effective alternative to traditional face-to-face provider appointments and examinations and a way to increase assess in areas of the state with shortages of health care professionals.
In response to the public health emergency caused by the spread of COVID-19, state policymakers suspended, through executive order, some of the barriers to telehealth in the private payer insurance market and in Medicaid. This flexibility increases access to care, which is especially meaningful for low-income individuals, families and children, pregnant women, the elderly, and people with disabilities who often have chronic conditions that continue to need monitoring. In effect, it puts Michiganders and their providers in direct control of how, when, and where they could assess care needs, as well as reduce in-person visits to only those who really needed them.
Michigan law allows health care providers to connect with patients via telemedicine, with some unwarranted restrictions. It requires the provider to be licensed in Michigan.
Michigan also has quite a bit of flexibility when it comes to telemedicine for Medicaid recipients, including those in the Healthy Michigan program. According to the Centers for Medicare and Medicaid Services, state policymakers can decide what types of telemedicine to cover; where in the state it can be covered; how it is provided/covered; what types of telemedicine practitioners/providers may be covered/reimbursed; and how much providers will be reimbursed.
In response to the COVID-19 pandemic, the Michigan Department of Health and Human Services gave Medicaid recipients increased freedom to use telemedicine. They were able to seek a consultation from their home or another convenient location, not just a health provider’s office or approved health facility.
Recommendation: Allow telemedicine across state lines and permanently allow Medicaid recipients to use telemedicine at home.
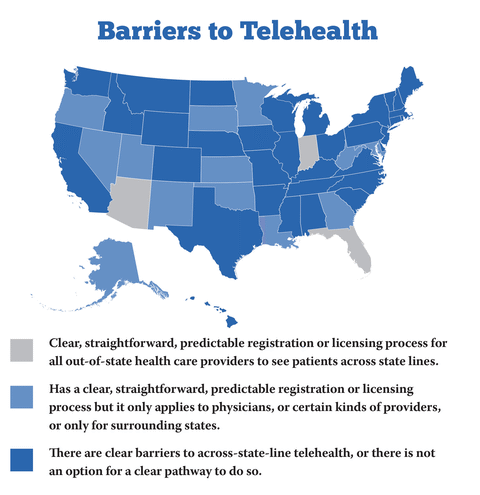
Some unwarranted restrictions prevent quality health care providers from across the country from connecting with and treating Michigan patients through telemedicine. Michigan lawmakers should update telemedicine licensing restrictions to allow health care providers to practice across state lines. Current law requires all providers to obtain a Michigan license. But this keeps high-quality providers from delivering needed care to millions of Michiganders and limits options and access for patients. Michiganders should be free to use telehealth to find the provider of their choice. This means that health care providers licensed and in good standing in their primary state of practice should be allowed to provide care within their scope of practice, regardless of where the patient might be.
In 2019, just 21 states allowed Medicaid recipients to see health providers through telemedicine at home. COVID-19 changed that, and 47 states updated their Medicaid telemedicine policies to permit telemedicine at home. Michigan policymakers should make this temporary pandemic policy permanent.
Michigan has many shortages of health professionals, including in primary care, mental health, and dental health. This change would help address these provider shortages, especially in rural areas. It would also help Michiganders with chronic conditions have additional choices to help manage them through remote providers and provide new business opportunity for Michigan-based providers.
Expanding telemedicine will improve health care access throughout all regions of the state, and it also better prepares Michigan for any future public health emergencies. The opportunity for innovation in health care through the expansion of telemedicine can help Michigan build a better, healthier future.
Overview of Michigan health professional licensing laws
Occupational licensing most often happens at the state level. It typically requires workers to complete approved educational programs, pass exams and pay fees.
In Michigan, the Department of Licensing and Regulatory Affairs (LARA) regulates 26 health professions under the Michigan Public Health Code. They include but are not limited to nurses, physicians, physician assistants, dentists, various mental health professional and pharmacists. Individuals who want to work the 26 regulated health professions must receive a Michigan-specific license before they can legally practice and treat patients.
Unfortunately, the licensing process is unnecessarily burdensome and costly, even for highly trained and highly skilled health professionals. Obtaining a license takes several weeks and more often months, depending upon the number of applicants in the pipeline.
This is especially troubling during a health emergency, like the COVID-19 pandemic. Unless a state of emergency is declared, much-needed health professionals located and licensed in other states with less urgent needs are unable to treat Michiganders without first getting a Michigan license.
But these unnecessary barriers are also a problem during nonemergency conditions. Many regions across our state have shortages of primary care, mental health and dental health professionals. These shortages leave those in need without care. Over time, this can lead to unaddressed illnesses, which may have been avoided or mitigated with more choices or more access.
Thankfully, many of the licensing requirements in the health industry are quite uniform between other states, making it easier to recruit those professionals. Professional licenses typically require a person to graduate from an accredited program, pass a national exam, take some amount of continuing education, and often obtain a national certification. Not only does this near uniformity make it easier to recruit already highly trained professionals to our state, but it opens the door to seeing more professionals through telemedicine.
Recommendation: Recognize the licenses of health care professionals who live in other states and have licenses in good standing.
The best way to reduce our shortage in health professionals and better prepare Michigan for any future public health emergencies is to recognize the licenses of health care professionals from other states if they are in good standing. That is, nurses, physicians, dental assistants, mental health professionals, and many other licensed specialists from elsewhere could diagnose and treat Michiganders. They would only need to have an existing license in good standing, been practicing for a few years, and have no ongoing investigations or previous suspensions.
Michigan already recognizes out-of-state licenses during times of disaster or when a professional attends to an ill or injured individual at the scene of an emergency. Michigan policymakers should extend this policy and apply it broadly. Doing so would improve access to more primary care professionals and specialists. Gov. Whitmer’s COVID-19 emergency order made this clear by allowing health professionals who are licensed and in good standing in any state to practice in Michigan without first getting a Michigan-specific license.
State policymakers should make the ideas of the emergency order permanent. Arizona and Pennsylvania both passed legislation to recognize the licenses of health care professionals from other states in 2019. They recognized the opportunity to eliminate costly red tape, attract much-needed workers, and promote new opportunities in their states. A streamlined licensing process for high-quality health care professionals in Michigan would address the shortage of providers during a health crisis and make relocating here or treating patients remotely more seamless.