The allure of national health insurance comes largely because it is perceived as successful in Canada and Britain. This thoroughly documented report shows conclusively that government-run national health insurance has led to serious and inevitable dilemmas that no country should want to emulate. The authors prove that other models have not been more successful than the U.S. in controlling costs or providing superior access to care, and that adoption of a national health system would have negative consequences. Released in cooperation with the Dallas-based National Center for Policy Analysis. 68 pages.
In virtually every country with national health insurance, politicians, health ministers, and other government officials are searching for ways to reform their health care systems. Increasingly, the reforms being adopted seek to replace socialism in medicine with privatization, competition and market incentives.
In 1989, the British government introduced radical market-based reforms in health care and began to allow private hospitals to compete against public hospitals for National Health Service funds. [1]
In 1987, the Netherlands introduced a voucher system which allows consumer choice among private and public insurance funds. [2]
In 1987, Germany introduced a new policy which encourages competition among hospitals. [3]
More recently, the government of New Zealand has signaled its intent to end 40 years of socialized medicine by giving people tax incentives to purchase private health insurance and by introducing market-based reforms in the public sector. [4]
Sweden, along with other European countries, has already introduced some "managed competition" into its national health insurance system, and with the recent change of government those reforms will undoubtedly continue. [5]
In Canada, pressures mount to allow private health insurance options and to institute user fees, and the father of Quebec's health care system (the oldest national health insurance scheme in Canada) has called for privatization and competition in the supply of health services. [6]
Russia's new health care reform plan calls for decentralization, "enterprise" and the introduction of financial incentives into health care. [7]
Chile has given its citizens financial incentives to opt out of national health insurance for the last decade, and most other Latin American countries are seeking ways to partially privatize their health care systems. [8]
As other countries struggle to reform their health care systems, they often look to the United States for guidance. Yet, many in this country are encouraging us to copy the health care system of some other country.
In Michigan, one prominent state representative has called for the state to copy Canada's "free and universal" care system. Many news reports suggest that our neighbor's socialized arrangement would be superior to any attempt at reforming our own. This study's heavy focus on Canada and its system, then,. is particularly timely and especially useful for the people and Legislature of Michigan.
National health insurance promises to make medical care a "right" and to grant all citizens equal access to it. But as this study shows, people in those countries which have adopted national health insurance are often denied access to modern medical technology, and the distribution of health care resources is far from equal. The special victims of national health insurance are the poor, the elderly, members of minority groups, and residents of rural areas.
This report does not focus on minor blemishes or easily correctable problems in the health care systems of other countries. Instead, it seeks an understanding of fundamental principles by identifying common patterns that tend to emerge in all countries with national health insurance and explaining why those patterns emerge inevitably from the politics of medicine.
As the United States wrestles with the problems of its health care system, it is tempting to look elsewhere for solutions. In general, countries with national health insurance spend less per person (and less as a percent of national income) on health care than does the United States. Those unfamiliar with other systems assume that the United States can control health care costs through national health insurance without any loss of benefits or deterioration of quality. In what follows, we briefly discuss this and other common myths about national health insurance.
The United States spends more on health care than any other country in the world, both in dollars per person and as a percent of gross national product (GNP). Does this mean that the United States, with a predominantly private system, is less able to control health care spending than are developed countries with national health insurance schemes?
As we shall see, international comparisons of health care spending are difficult, not least because of differences in measuring techniques. But first we should note that the United States is wealthier than other countries. Almost without exception. countries with more income spend more on health care. In fact. health economists have discovered that 90 percent of the variation in, health care spending among developed countries is based on income alone. [9]
This should give pause to anyone who believes the United States will significantly lower health care spending by adopting the system or institutions of some other country. Apparently, as people have more income, they spend more on health care, whether their spending takes place through the market, the political system or quasi-public institutions.
United States vs. Canada: Growth in Spending.
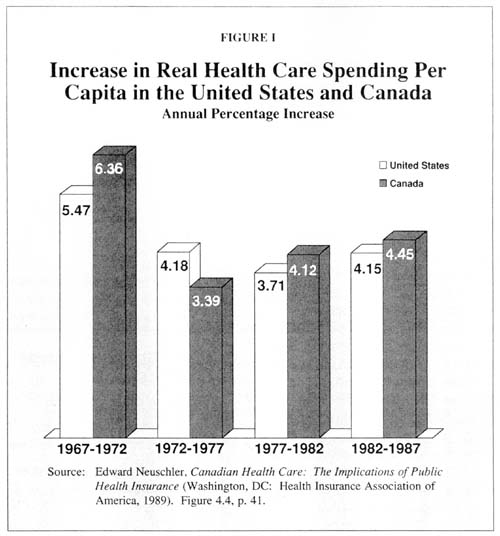
Let's take a closer look at the United States and Canada, whose health care system is often held up to us as a model. In 1987, the United States spent $2,004 per person on health care, whereas Canada spent only $1,520. Some people argue that if the U.S. adopted Canada's health care system, it could cut health care spending by 25 percent. They buttress their argument by looking at the record over time. In 1967, the United States and Canada spent virtually identical proportions of GNP on health care (6.33 percent in the United States, and 6.38 percent in Canada). Canada's system of national health insurance was implemented between 1968 and 1971. Since then the U.S. has surged ahead. In 1987, the United States spent about 11.1 percent of its GNP on health care, whereas Canada spent only 9.0 percent. [10]
The problem with those comparisons is that health care spending as a percent of GNP is a fraction. If the fraction grows over time, we need to know whether the growth is being caused by changes in the numerator (health care spending) or in the denominator (GNP). As it turns out, the above differences can be almost totally explained by the behavior of the denominator. Over the 20-year period (1967 to 1987), Canada's real GNP per capita grew 74 percent, while the U.S. figure grew only 38 percent. [11] If we look at health care spending alone, rather than its relationship to GNP, we discover that:
Before Canada implemented its system of national health insurance, the country
was spending 75 percent of what the United States spent on health care per
person.
In 1987, Canada continued to spend 75 percent of the U.S. level.
Over the 20-year period, real increases in health care spending per capita have
been virtually the same in both countries. (The increase was 4.38 percent in the
United States versus 4.58 percent in Canada.)
Canada has been no more successful than the United States in controlling health care spending. As Figure I shows, in recent years it has been less successful. [12]
United States vs. Canada: Levels of Spending.
There are other problems in comparing United States and Canadian health care spending:
First, the Canadian number doesn't include capital spending to the same extent
that the U.S. number includes it.
Second, the U.S. number includes research and development (R & D) costs. Canada
engages in very little R & D spending, while U.S. R & D spending results in
technological innovations that benefit Canada as well as the rest of the world.
Third, the U.S. population is slightly older, and older people inevitably
consume more health care.
According to one study, correcting for these
differences between the two countries cuts the gap in the fraction of GNP spent
on health care in half.
[13]
Other adjustments also must be made. In both countries, the costs of administering government health care spending are largely hidden. For example, the cost of collecting tax dollars to pay for health care does not show up in the health care budgets of either country, whereas the cost of collecting private insurance premiums is counted as part of U.S. health care costs. Similarly, auditing expenses are usually included in the budgets of other public agencies. But since Canada's public sector is relatively larger than that of the United States, far more of Canada's costs are buried in bureaucratic budgets.
United States vs. Canada: Differences in Health Care Needs.
Because of historical and cultural differences between the two countries, the need for health care spending is often higher in the United States than in Canada. For example, the United States has a much higher violent crime rate, heavier illegal drug use and a greater incidence of AIDS – all of which generate more health care spending. According to Leroy Schwartz (Health Policy International): [14]
The U.S. male homicide rate is five times that of Canada, and for every homicide
there are 100 assaults reported to hospital emergency rooms.
The U. S. rate of incidents of AIDS is three times that of Canada, and the
lifetime cost of treatment is about $85,000 per patient:
More than 25 percent of the 10,000 to 15,000 annual spinal cord injuries in the
United States are due to violent assaults, and treatment and rehabilitation
costs are about $600,000 per patient.
There are about 375,000 drug-exposed babies in the United States with an average
treatment cost of $63,000 per baby. This problem is
negligible in Canada.
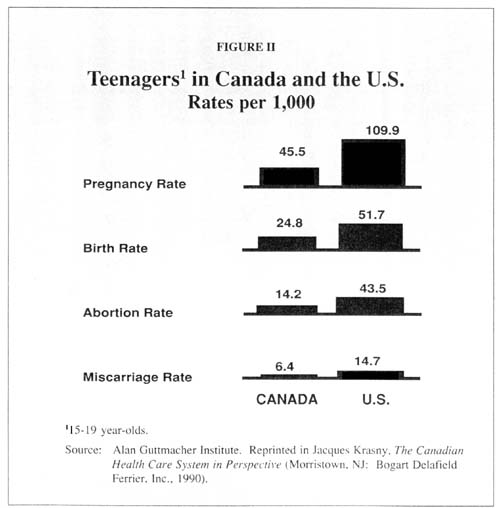
The United States also has health care costs related to war injuries (including those of Vietnam veterans), which Canada does not have. And Figure II illustrates another important difference: U.S. teenage women have almost 2 1/2 times the pregnancy rate of teenagers in Canada, twice the birthrate, about three times the abortion rate and more than twice the miscarriage rate. Because teenage mothers are more likely to have premature babies and other complications, these differences cause higher health care spending in the United States.
Other Comparisons.
No one has tried to sort out these differences to arrive at a bottom line. But there is considerable anecdotal evidence that the real cost of U.S. health care may actually be lower than Canada's. For example, hospitals in British Columbia contract with U.S. hospitals across the border in Seattle to perform heart surgery on Canadian patients. [15] There is a similar arrangement between Ontario hospitals and those in Detroit. Canadian hospital managers apparently have concluded they make a "profit" on these transactions, and at the same time reduce the public outcry over long waiting lists.
Another way of comparing the two nations' health care costs is to compare Canada with some of the largest HMOs in the United States. The "managed care" programs of HMOs resemble the cost controls imposed in Canada in the sense of a commitment to control spending. Moreover, some HMOs are as populous as Canadian provinces. About half of Canada's provinces have a population of one million or fewer people, while seven HMOs in the United States have more than one million. Although people enrolled in HMOs may not be a random sample of the U.S. population, Figure III shows that large HMOs in the United States have lower costs per person than Canada has:
The Harvard Community HMO in Massachusetts spends only 73 percent as much per
person as Canada spends.
Both the Kaiser Permanente and Cigna HMOs spend about 65 percent as much per
person.
To summarize, we can draw at least four important conclusions. 1) There is no evidence that Canada has done a better job than the United States at controlling health care spending overtime. 2) Canada's spending on health care – under both a private and a public system – consistently has been about 75 percent of what the United States spends. 3} Although international statistics show that the United States spends more per capita on health care than Canada, these statistics can be very misleading. 4) There is some evidence that U.S. health care is less expensive when the comparison is made on a more level playing field.
The United States vs. Other Developing Countries.
In comparing United States health care with that of other developed countries, we encounter the same difficulties. In addition, most international statistics on health care spending are produced by the Organization for Economic Cooperation and Development (OECD). Yet because of differences in reporting standards of different countries, OECD statistics are not always reliable. [16]
Table I shows the results of an attempt to develop more accurate health care spending measurements among OECD countries:
Using more precise
measuring techniques, we find that the United States spends more of its income
on health care than other countries – but the difference is smaller than people
commonly believe.
During the 1980s, the real growth rate for health care spending was higher in 11
of 15 countries than in the U.S.
In per capita terms, most countries had real growth rates that were more than
double the U.S. rate.
Many believe that countries with national health insurance have an "advantage" the U.S. health care system does not. In those countries the government can, in principle. limit health care dollars and tell hospital managers to ration the money they are given to spend. But that power is more apparent than real, and politicians who exercise it risk being replaced by their competitors. In the political systems of other countries, as in the U.S., there is unrelenting pressure to spend more on health care.
This myth is often supported by reference to two facts: that life expectancy is not much different among the developed countries and that the U.S. infant mortality rate is one of the highest among developed countries.
Mortality Rates and Health Care.
General population mortality rates tell us almost nothing about the efficacy of health care systems because, throughout the developed world, there is almost no relationship between health care and general mortality – either among or within countries. General mortality rates are far more closely related to socioeconomic factors and lifestyle.
For example, in Sweden, there are striking differences in health outcomes between Stockholm and Hollard, a rural, agricultural area in the nation's south: [17]
Infant mortality in Stockholm is almost twice as high as in rural Hollard, and mortality among 40-year-olds in Stockholm is 50 percent higher.
Even the
middle-class suburban area outside of Stockholm city has an infant mortality
rate 71 percent higher than Hollard's.
Yet no one has
seriously claimed that these differences are the result of the Swedish health
care system.
In Norway, people in the urban areas of Oslo and Akershus have the most contacts with physicians. But infant mortality in those areas is still higher than in, say, Hordaland in western Norway. [18] In virtually every country, there is a positive relationship between income and health status and between social class and health. Lifestyle also appears to matter. For example, in Norway, children born to unmarried women between 1971 to 1975 had a 55 percent higher (perinatal) mortality rate than children born to married women. Between 1976 and 1980, the rate for unmarried women was 40 percent higher. [19]
Where Health Care Makes a Difference.
A population's general mortality is affected by many factors over which doctors and hospitals have little control. For those diseases and injuries modern medicine can affect, however, it makes a big difference where a patient lives. For premature babies, for children born with spina bifida or for people who have cancer, a brain tumor, heart disease or chronic renal failure – the chances of survival are best in the United States.
Access to Modern Medical Technology in Canada.
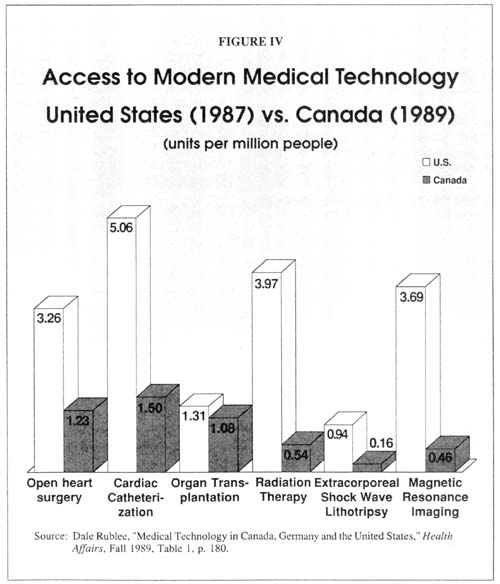
Figure IV compares the availability of modern medical technology in the United States and Canada. As the figure shows:
On a per capita basis,
the United States has eight times as many magnetic resonance imaging (MRI) units
– which use magnetism instead of x-rays – as Canada.
The United States has seven times as many
radiation therapy units (to treat cancer) per person.
The United States also
has about six times as many lithotripsy units (to destroy kidney stones and
gallstones with sound waves) per person.
And, per capita, the
United States has about three times as many open-heart surgery units and cardiac
catheterization units (for the treatment of heart disease).
Note that the figures contrast the United States with Canada two years later. Contrasting the two countries in the same year would reveal an even greater disparity. While critics of the U.S. health care system claim that we have too much technology, all the evidence suggests that Canada has too little – as a result of the conscious decisions of government officials. Doctors in British Columbia have taken out full-page newspaper advertisements warning that their patients' lives are endangered by government's refusal to purchase lifesaving medical technology. It is easy to understand why these and other Canadian doctors are complaining. Consider what the shortage of diagnostic equipment means for patients: [20]
Seattle, Washington (pop. 490,000) has more computerized axial tomography (CAT) scanners (used, for example, to detect brain tumors) than the entire province of British Columbia (pop. 3 million).
There are more MRI scanners in Washington state (pop. 4.6 million) than in all of Canada (pop. 26 million).
The province of Newfoundland (pop. 570,000) has only one CAT scanner, causing patients who need a CAT scan to wait an average of two months.
Prince Edward Island (pop. 128,000) has no CAT scanner, and patients who need a CAT scan must leave the province in order to obtain one.
Because of a shortage of laboratory testing equipment in 1988, women in Newfoundland waited up to five months for a Pap smear (needed to detect cervical cancer) and two months for an "urgent" Pap smear.
Also because of an equipment shortage, women in Newfoundland waited as long as 2-1/2 months for a mammogram (used to detect breast cancer).
Women on Prince Edward Island wait from four to eight months for mammograms, and even "emergency" patients can wait as long as one month.
Access to Modern Medical Technology in Britain.
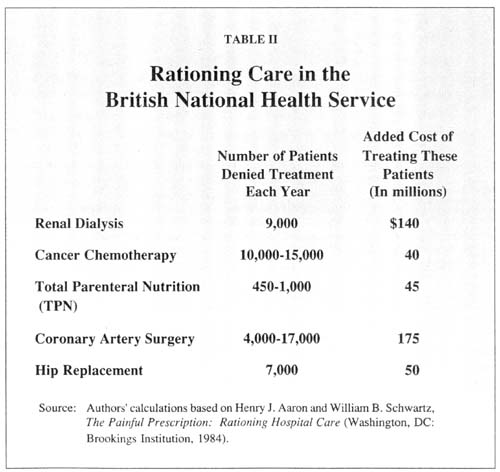
In an extensive study of Britain's National Health Service (NHS), Brookings Institution economists estimated the number of British patients denied treatment each year, based on U.S. levels of treatment. Most of the patients suffered from life-threatening diseases and the denial of treatment meant certain death. Table II presents these estimates, along with estimates of what it would cost the NHS to bring British treatment up to U.S. standards. As the table shows:
Each year, about 9,000 British kidney patients fail to receive renal dialysis or
a kidney transplant – and presumably die as a result.
As many as 15,000
cancer patients and 17,000 heart patients fail to receive the best treatment
modern medicine can offer.
As many as 1,000
British children fail to receive lifesaving total parenteral nutrition (TPN)
therapy and about 7,000 elderly patients are denied pain-relieving hip
replacements.
Willingness to Adapt to New Technology.
Some argue that countries with national health insurance delay the purchase of expensive technology in order to see if it works and is cost-effective. If true, the downside of this approach is that patients are denied access to lifesaving treatment while government bureaucracies evaluate it.
During the 1970s, for example, lifesaving innovations were made in kidney dialysis, computerized axial tomography (CAT) scanning and pacemaker technology. Yet as Table III shows: [21]
The rate of implants of pacemakers in the United States during the mid-1970s was
more than four times that of Britain and almost 20 times that of Canada.
CAT scanners in the United States were more than three times as available in the
United States as in Canada and almost six times as available as in Britain.
The treatment rate of kidney patients in the United States was more than 60
percent greater than in Canada and Britain.
There is considerable evidence, however, that cost-effectiveness is not what drives the bias of other governments against modern medical technology: [22]
CAT-scan technology was invented in Britain, and
until recently Britain exported — probably with government subsidies — about
half the CAT scanners used in the world. Yet the British government has
purchased only a handful of the devices for the National Health Service and has
even discouraged private gifts of CAT scanners to the NHS.
Britain also was
the codeveloper of kidney dialysis, a lifesaving method of treating patients
with chronic renal failure, yet Britain has one of the lowest dialysis rates in
Europe.
One could argue that the "need" for technology varies from country to country. For example, the incidence of chronic renal failure may be higher in the United States than in other developed countries. Even if this were true, however, a comparison of Tables III and IV shows that every country had substantially increased the number of patients being treated by 1984, when even East Germany was treating more patients than Britain or Canada had treated eight years earlier.
The Politics of Medical Technology.
It would be a mistake, however, to think of the current U.S. health care system as ideal. The United States has not always been the first country to adopt new technology (even technology that works and is cost-effective). We do not always purchase the most technology. And we have not always made cost-effective choices among competing technologies.
In 1970, before a dialysis benefit was extended to the entire population under Medicare, the U.S. treatment rate for patients with renal failure was on a par with Britain's and less than half that OTSweden and Denmark. Only after Medicare provided a virtual blank check did the U.S. treatment rate soar. [23]
How we treat kidney patients was also dictated by government reimbursement policies. Studies show that home dialysis is less expensive than dialysis in a hospital or a clinic and prior to the Medicare expansion, about 40 percent of U.S. dialysis treatment was home-based. But because Medicare gave physicians incentives to avoid home-based dialysis, the rate fell to 12 percent by 1978. There is also evidence that kidney transplants are more cost-effective (over the long run) than dialysis. But because Medicare reimbursement policy favored dialysis, the United States was 12th of 20 developed countries in the percent of kidney patients treated by transplant in 1985. [24]
A more recent technological innovation is extracorporeal shock wave lithotripsy (ESWL) to disintegrate kidney stones and gallstones and eliminate the need for surgery. In 1989, the U.S. rate of lithotripters per capita was exceeded by rates in Germany (where ESWL was invented) and Belgium. [25]
Overall, the best way to think about government policies toward technology is in terms of the politics of medicine. As the role of government expands, health care tends to evolve from a pro-technology phase to an antitechnology phase. In the first stage. government tends to spend on items perceived as under-provided by the market or by conventional health insurance. Thus. practically every less-developed country has used government funds to build at least one modern hospital, usually in the largest city. and to stock it with at least one example of each new technology — even though the vast majority of citizens lack basic medical care and public sanitation.
As government's role in medicine begins to expand, more and more interest groups must be accommodated. In this stage, government policy tends to be antitechnology because the small number of people who need the technology are so heavily outnumbered. Along the way, these general trends may be violated with respect to any particular technology because of the varied, even random, ways in which special interest pressures are exerted. We analyze the politics of medicine in more detail below.
When the United States had a pure cost-plus health care system, technology tended to be adopted quickly because physicians – unconstrained by considerations of cost – found the technology useful. When the role of government was minimal, it was easier to acquire public funds where conventional insurance coverage was lacking (e.g., kidney dialysis and organ transplants). It is not surprising that the United States made great use of technological innovations.
Our experience in the future may be very different, however. In the United States we pay more for health care. We also get more. And what we get may save our lives. But increasingly, our health care system is acquiring the characteristics of the health care systems of other countries, in which access to medical technology is determined by rationing and politics. [26]
Virtually every government which has established a system of national insurance has proclaimed health care to be a basic human "right." Yet far from guaranteeing that right, most national health systems routinely deny care to those who need it. Not only do citizens have no enforceable right to any particular medical service, they don't even have a right to a place in line when health care is rationed. The 100th person waiting for heart surgery is not "entitled" to the one hundredth surgery, for example. Other patients can, and do, jump the queue for any number of reasons.
By U.S. standards, one of the cruelest aspects of government-run health care systems in other countries is the degree to which these systems engage in non-price rationing. Take the health care systems of Britain and New Zealand, for example. In both countries, hospital services are completely paid by government. Both also have long waiting lists for hospital surgery:
In Britain, with a population of about 57
million, the number of people waiting for surgery is more than one million.
[27]
In New Zealand, with a population of
three million, the waiting list is more than 50,000.
[28]
In Canada, with a population of about 25
million, the waiting list is more than 250,000.
[29]
On the surface, the number of people waiting may seem small relative to the total population – ranging from 1 percent in Canada to almost 2 percent in Britain. However, considering that only 16 percent of the people enter a hospital each year in developed countries [30] and that only about 4 percent require most of the serious (and expensive) procedures, [31] these numbers are quite high. [32] In New Zealand, for example, there is one person waiting for surgery for every three surgeries performed each year. [33]
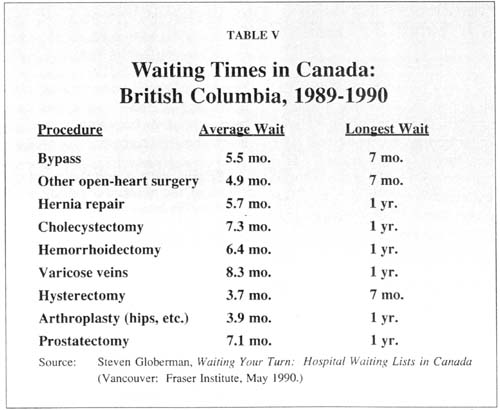
In Britain and New Zealand, elderly patients in need of a hip replacement can wait in pain for years, and those awaiting heart surgery often are at risk of their lives. Perhaps because Canada has had a national health care program for only half as long, the rationing problems are not as great as they are in Britain and New Zealand, although all three countries have similar cultures. But because the demand for health care has proved insatiable, and because Canadian provincial governments severely limit hospital budgets, the waiting lines for surgery and diagnostic tests are growing:
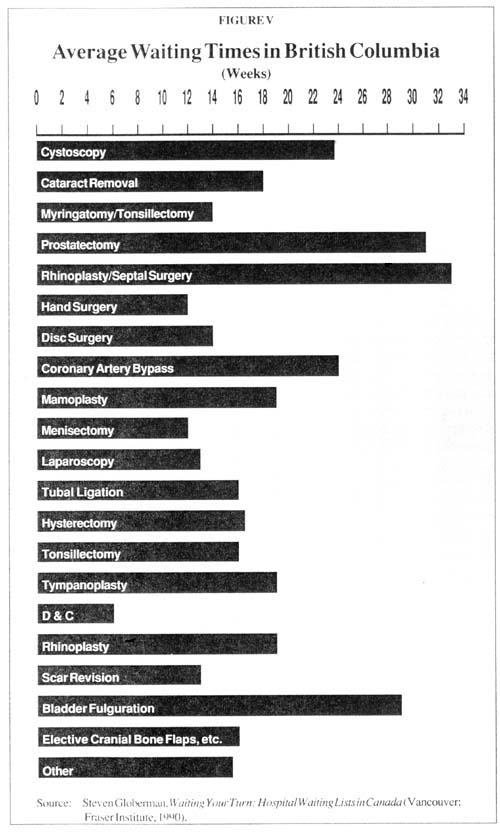
As Table V and Figure V show, patients in British Columbia wait up to a year for
routine procedures such as cholecystectomies, prostatectomies, hip replacements
and surgery for hemorrhoids and varicose veins.
In Ontario, patients wait up to six months for a CAT scan, up to a year for eye
surgery and orthopedic surgery, up to a year and four months for an MRI scan and
up to two years for lithotripsy treatment.
[34]
All over Canada, patients wait for coronary bypass
surgery, while the Canadian press tells of heart patients dying on the waiting
list.
[35]
The defenders of national health insurance often point to the low level of health care spending in other countries as "proof" of efficient management. Nothing could be further from the truth. By and large, countries that have slowed the growth of health care spending have done so by denying services, not by using resources efficiently.
How much does it cost a hospital to perform an appendectomy? Outside the United States, it is doubtful that any public hospital knows. Nor do government-run hospitals typically keep records that would allow anyone else to find out. [36] One reason why Margaret Thatcher called for systematic health care reform was that even Britain's best hospitals did not have computerized records, and it was not uncommon for the head of a hospital department to be unaware of how many people the department employed. In organizational skills and managerial efficiency, the public hospitals of other countries are far behind hospitals run by Hospital Corporation of America, Humana or American Medical International.
More often than not, government-run hospitals in other countries are disastrously inefficient. It is not unusual to find a modern laboratory and an antiquated radiology department in the same hospital. Nor is it unusual to find one hospital with a nursing shortage near another with a nursing surplus. Where excellence exists, it usually is distributed randomly – often the result of the energy and enthusiasm of a few isolated individuals rather than decisions by hospital managements.
Moreover, even when specific inefficiencies are acknowledged, it is often impossible to eliminate them because of political pressures. For example, health economist Alain Enthoven reports that "it is more difficult to close an unneeded [British] hospital than an unneeded American military base." [37]
What about bed management? Consider that:
While 50,000 people
wait for surgery in New Zealand and the waiting lists grow in Canada, at any
point in time one in five hospital beds is empty.
[38]
While one million
people wait for surgery in Britain, at any point in time about one in four
hospital beds is empty.
[39]
Moreover, in Britain, New Zealand and
Canada, about 25 percent of all acutecare beds are occupied by chronically ill
patients who are using the hospitals as nursing homes – often at six times the
cost of alternative facilities.
[40]
In Canada, hospitalized chronic patients are known as "bed blockers," and they are apparently blocking beds with the approval of hospital administrators – who may believe that such patients, because they use mostly the "hotel" services of the hospital, are less of a drain on limited hospital budgets. [41]
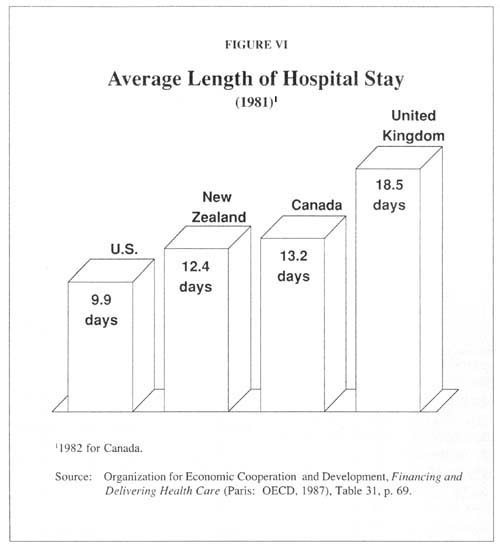
One widely used measure of hospital efficiency is average length of stay. In general, the more efficient the hospital, the more quickly it will admit and discharge patients. By this standard, U.S. hospitals are far in front of their international rivals. [42] As Figure VI shows: [43]
The average hospital stay is 39 percent longer in New Zealand, 42 percent longer in Canada and 61 percent longer in Britain.
The average hospital stay among all OECD countries is 76 percent longer than in the United States.
Almost all health care economists agree that widespread inefficiencies exist in the U.S. health care system. But we will not improve our efficiency by adopting the practices of other countries.
One of the most surprising features of European health care systems is the enormous amount of attention given to the notion of equality and the importance of achieving it. Aneurin Bevan, father of the NHS, declared that "everyone should be treated alike in the matter of medical care." [44] The Beveridge Report, a blueprint for the NHS, promised "a health service providing full preventive and curative treatment of every kind for every citizen without exceptions." [45] The British Medical Joumal predicted that the NHS would be "a 100 percent service for 100 percent of the population." [46]
The goal of NHS founders was to eliminate inequalities in health care based on age, sex, occupation, geographical location and – most importantly – income and social class. As Bevan put it, "the essence of a satisfactory health service is that rich and poor are treated alike, that poverty is not a disability and wealth is not advantaged." [47] Similar statements have been made by politicians in virtually every country that has established a national health insurance program.
Inequality in Britain.
Such rhetoric rarely relates to the facts. Britain's ministers of health have long assured Britons that they were leaving no stone unturned in a relentless quest to root out and eliminate inequalities in health care. But, although an unofficial government campaign tried to suppress it, an official task force report (the Black report) concluded that there was little evidence of more equal access to health care in Britain in 1980 than when the NHS was started in 1948. [48] Virtually every scholarly study of the issue has pointed to a similar conclusion. [49] For example
One study of health care spending across geographical areas of England found no
relationship between any measure of medical need and the amount spent.
[50]
Another study found that people in Britain's highest social class received 40
percent more medical care (in relation to their need for it) than people in
Britain's lowest social class.
[51]
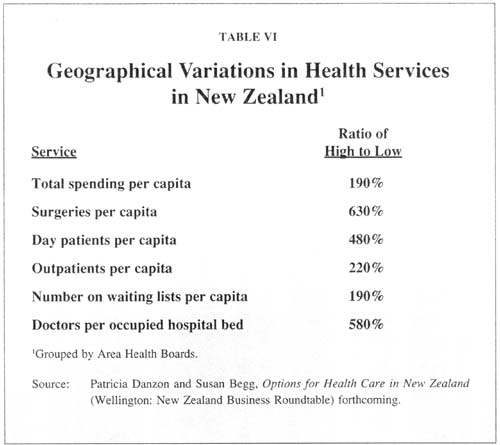
Other studies have documented widespread inequalities in health care in Sweden, [52] Canada, [53] New Zealand [54] and elsewhere. For example, New Zealand's health care system is virtually identical to Britain's and the goal of equal access to health care ranks just as high. Yet as Table VI shows:
Among the geographical regions of New Zealand, spending on health care per
person varies by a factor of almost two to one.
Surgeries per capita vary by a factor of more than six to one, doctors per
occupied bed by almost six to one and the number of patients waiting for surgery
by almost two to one.
Inequality in Canada.
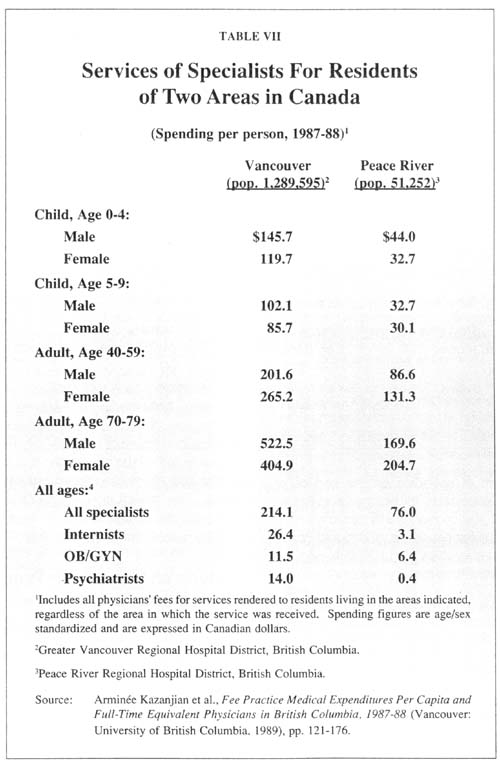
Canada is another country that puts a high premium on equality of access to medical care. if the official rhetoric is to be believed. How well have the Canadians done? Table VII compares the amount of spending on the service of physician specialists for two areas in British Columbia: Vancouver, the largest city with a population in excess of one million, and Peace River, a rural area of about 51,000. As the table shows:
Residents of Vancouver receive about three times more specialist services per
person than residents of Peace River, and this inequality holds for both males
and females across all age groups.
The differences are even more striking for specific specialties, with an eight-toone
difference in the services of internists and a 35-to-one difference in the
services of psychiatrists.
One might suppose that the lower level of specialist services in Peace River would be offset by a higher level of general practitioner (GP) services. That is not the case. As Figure VII shows, Vancouver residents also enjoy about 50 percent more GP services.
Effects on Low-Income Families.
There is substantial evidence that when health care is rationed, the poor are pushed to the rear of the waiting line. In general, low-income people in almost every country see physicians less often, spend less time with them, enter the hospital less often and spend less time there – especially when the use of medical services is weighted by the incidence of illness. In Canada [55] and other countries with national health insurance. there is no national waiting list to assure that the sickest people get care first. Even in the same hospital there are instances where elective patients get surgery while those in much greater need are forced to wait. [56] Moreover, anecdotal evidence suggests that the wealthy and powerful do not wait as long as others. As one study of the Canadian system noted:
"Critics charge that those who are rich, influential, or 'connected' often 'jump the queue,' which changes Canadian health care into a two-tiersystem – precisely what the government wanted to avoid." [57]
Interestingly, among the patients who jump the queue in Canada are Americans who pay out-of-pocket for care. U.S. patients add to hospital revenues, so hospital administrators value them. Since Canadians cannot legally pay for care at a national health insurance hospital, the typical Canadian patient must wait in line. [58]
How does access to health care for low-income people in the United States compare with access in countries with national health insurance? Our poorest citizens – those on Medicaid – probably have more access to better health care than low-income citizens in any other country. Being on Medicaid usually means access to all the technology of the U.S. health care system; such technology is more available in the United States, and Medicaid will usually pay for it. Even though Medicaid rationing is becoming more prevalent, the U.S. probably has far less rationing than most other countries.
International opinion surveys show that, in the U.S., 7.5 percent of people say they do not receive needed care for financial reasons compared to only 0.6 percent in Canada and 0.1 percent in Britain. A somewhat smaller percent of people in the United States (5.1 percent), but a much larger percent in Canada (3.1 percent) and Britain (4.6 percent) say they cannot get care for nonfinancial reasons, including inability to get an appointment, unavailability of services, lack of transportation, etc. [59]
It is not clear what these responses mean. In the United States we more frequently ask people to choose between money and health care. In Britain and Canada, people more frequently must choose between health care and other (rationing) costs. We do not know if those surveyed would have obtained health care if they had perceived their medical needs as being more urgent. However, that must have been the case quite often. Two-thirds of the people in the United States who said they did not get needed care for financial reasons had health insurance. [60]
A different way of comparing the United States and Canada is to look at medical care received by income group. As Table VIII shows, the differences are not that great. Low-income Canadians make more trips to physicians, but low-income Americans are slightly more likely to spend time in a hospital.
In every country, some people slip through the social safety net. But for the most part, the United States has already achieved the goal of socialized medicine: the removal of financial barriers to health care. And, considering the rationing of medical technology in countries with national health insurance, the U.S. health care system may have gone further in removing barriers to medical care than any other country in the world.
Most people in Britain, Canada and other countries that ration health care believe that the wealthy, the powerful and the sophisticated move to the head of the rationing lines. Because government officials have little interest in verifying this fact, few formal studies exist. There is considerable evidence, however, that in the face of health care rationing those who can pay find other ways to obtain health care.
In response to severe rationing by waiting, both Britain and New Zealand have a growing market in private health insurance – where citizens willingly pay for coverage for private surgery, although they are theoretically entitled to "free" surgery in public hospitals. As a result, the privately insured pay for health care twice – through taxes and through insurance premiums.
In Britain, the number
of people with private health insurance policies has more than doubled in the
last ten years, currently totaling about 10 percent of the population with about
one in every five elective surgeries performed in the private sector.
[61]
In New Zealand,
one-third of the population is covered by private health insurance, and private
hospitals now perform 25 percent of all surgical procedures.
[62]
Since Canada does not allow private health insurance, if Canadians go to the less than 1 percent of the private physicians or less than 5 percent of private hospitals, they must pay the full bill out-of-pocket. [63] An exception is thesmall number of outpatient surgery clinics operated by entrepreneurial physicians. Government will pay the surgeon's fee but not other costs. Canadians who receive cataract surgery on an outpatient basis, for example, must pay from $900 to $1,200 out of pocket.[64]
In addition, Canadian citizens are increasingly entering the United States to get health care they cannot get at home. In some cases, the Canadian province pays the bill. In other cases, patients spend their own money. [65] In either event, patients must bear the costs of travel. For example:
About 100 Canadian heart patients go to the Cleveland clinic each year because
they cannot get timely treatment in their own country.
[66]
A volunteer organization, "Heartbeat Windsor," arranges for Ontario heart
patients to get treatment at Detroit hospitals (which accept the Ontario rate as
payment in full), and Alberta has indicated it will accept a similar
arrangement.
[67]
Because there is only one lithotripter in all of Ontario, many lithotripsy
patients cross the border; at Buffalo General Hospital in New York, for example,
half of the lithotripsy patients are Canadians.
[68]
Because of the inadequate facilities in Canada, about half of the in vitro
fertilization patients at the University of Washington Medical Center are
Canadians, paying $5,000 out of pocket for each procedure.
[69]
In general, the Ontario government will pay 75 percent of the standard U.S. hospital charges and the same physician's fee it would have paid had the service been provided in Ontario. Apparently many American hospitals and physicians believe they can make a profit at those rates. U.S. drug dependency centers are actually marketing their services to Canadian citizens. Although the number of Canadian patients who cross the border is small, it is growing: [70]
In 1990, the Ontario Health Insurance Plan paid about $214 million to U.S.
doctors and hospitals – up 45 percent over the previous year.
Of that amount, 40 percent went to Florida, 9 percent to New York, 5 percent to
Michigan and Minnesota and 4 percent to California.
Americans have been repeatedly told that at least in Canada's health care system the quality of care has not suffered because of national health insurance. Yet there are increasing reports by doctors and the news media of patient deaths and near-deaths, precisely because of the government's limits on access to technology and the resulting health care rationing. Here is one doctor's report of what conditions are like in Quebec:
"In my academic practice at a teaching neurologic hospital in Montreal, the wait for the treatment of a "minor" medical problem (e.g., carpal tunnel syndrome) could be half a year or longer. What I considered essential services were unavailable. I recall losing an argument with the radiologist on call over whether a patient with a new stroke should have a CT scan at 5:05 p.m.; he judged that the situation was not an emergency serious enough to warrant performing the procedure after regular hours." [71]
Among the victims of Canada's system of health care rationing are the following wellknown cases:
Malcolm Stevens of British Columbia died of a heart attack after two months on
the waiting list. Ironically, that same day his doctor bumped another patient
from the surgery schedule in order to make room for Stevens.
[72]
Charles Coleman, a 64-year-old man, died shortly after a heart operation at
Toronto's St. Michael's Hospital. Coleman's operation had been postponed 11
times.
[73]
Stella Lacroix's death started as a suicide. Moments after she swallowed a quart
of cleaning fluid she raced to the
nearest emergency room. Because the hospital wasn't equipped to perform the
surgery she needed to stop the internal bleeding, the emergency room physician
spent 3 1/2 hours contacting 14 hospitals in an effort to secure emergency
surgery and an available intensive care bed. By the time she arrived at York
Country Hospital, in Ontario, it was too late. She died that night.
[74]
In January 1990, two-year-old Joel Bondy needed urgent
heart surgery that was repeatedly postponed. Alarmed at their son's
deteriorating condition, his parents contacted Heartbeat Windsor, an underground
railroad for Canadian heart patients, to arrange for the surgery in Detroit.
Embarrassed by media coverage of Joel's situation, Canadian officials promised
Joel would be moved to the top of the waiting list. After a fourhour ambulance
ride to a hospital which lacked an available bed, the family had to spend the
night in a hotel. The next day Joel Bondy died.
[75]
These examples are far from unique. Indeed, the Canadian press has produced scores of similar stories. The following are some additional examples:
According to one
report, 24 people died in 1989 while waiting for heart surgery in British
Columbia.
[76]
At Winnipeg's Health
Science Center, Manitoba's largest hospital, six heart patients died in 1988
before they reached the operating room.
[77]
In Toronto, where
about 1,000 people are facing waits as long as a year for bypass surgery at
three hospitals, two patients died in two months.
[78]
In January 1989, long
waiting lists forced Toronto's highly respected Hospital for Sick Children to
send home 40 children who needed heart surgery.
[79]
At Moncton Hospital in
New Brunswick, some patients were kept in hallways and even in closets, while
2,300 people were on the waiting list for surgery.
[80]
Because of a
four-month wait for mammograms at St. Clare's Hospital in Newfoundland in 1988,
preventive screening became impossible and the hospital could handle only women
who needed an immediate diagnosis.
[81]
In September 1989,
Princess Margaret Hospital in Toronto announced it would not accept new cancer
patients requiring radiation therapy for a six-week period in order to clear up
a 300- patient backlog.
[82]
In 1990, the only
hospital doing cardiovascular surgery in northern Alberta had 210 adults and
children on its waiting list – with some patients waiting as long as a year.
[83]
In 1989, doctors at
Brandon General Hospital said bed closings had left 91 patients, including
cancer victims, waiting up to six weeks for urgent surgery. Most of the patients
had cancer of the breast, large bowel or lungs.
[84]
In 1989, the Health
Minister of Newfoundland announced the closure of more than 400 beds due to lack
of funds – one-eighth of all beds in public general hospitals in the
province.
[85]
In an interview with
reporters on a Canadian Broadcasting Company program, ambulance drivers
recounted how a patient's condition steadily deteriorated as they traveled from
one emergency room to another in search of one that would take him. The patient
died.
[86]
A frequent criticism of the U.S. health care system is that it is wasteful because a considerable number of procedures are "unnecessary." For example, Dr. Robert Brook of the Rand Corporation maintains that "perhaps one-fourth of hospital days and two-fifths of medications could be done without." [87]
One source of evidence for unnecessary medical care is a series of studies that show wide variations in the rate of treatment among different U.S. communities, with no apparent justification. Another major study of unnecessary medical procedures, conducted by the Rand Corporation, concluded that 40 percent of medical procedures were inappropriate" or "questionable." [88]
One might suppose that in countries where health care is rationed and many medical needs are unmet, doctors would tend to provide only "necessary" care. That turns out not to be the case. As in the United States, considerable variation in treatment rates exists in countries with socialized medicine. For example, in Britain there are widespread differences in the referral (to specialists) rates of general practitioners and in their prescribing habits:
One study found a
four-to-one difference in the number of prescriptions per patient among British
doctors, and for prescriptions to treat specific diseases the differences were
even greater.
[89]
The difference in the
rate at which British general practitioners refer patients to hospital
specialists varies by at least four to one – according to one study by 25 to one
– and there is a high correlation between referrals and subsequent hospital
admissions.
[90]
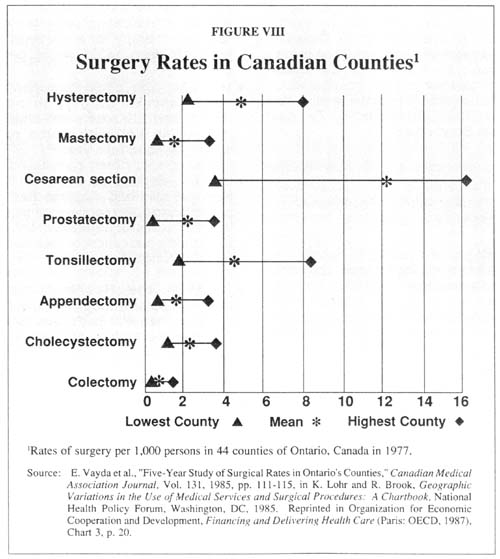
Figure VIII shows that the practice patterns of physicians vary widely in Canada as well. For example:
There is a four-to-one
difference among Canadian counties in the rate of cesarean sections.
There is a four-to-one
difference in rates of tonsillectomy and hysterectomy and a twoto-one
difference in the rates of mastectomy, prostatectomy
and cholecystectomy.
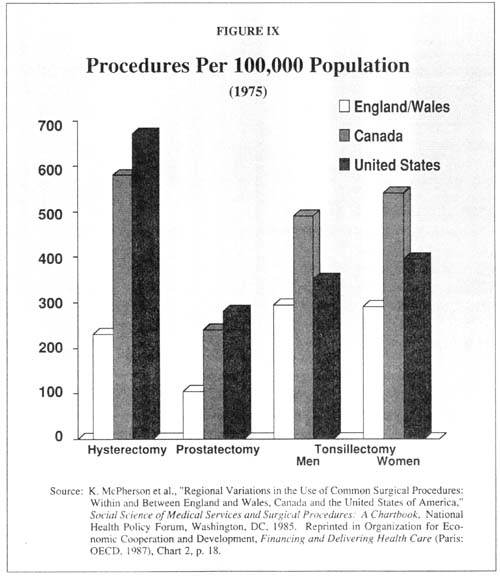
Figures IX and X compare the rates for surgeries for which it is believed that doctors exercise a great deal of discretion. There is no common pattern except that British rates are generally lower – as they are for almost all types of surgery.
Close inspection of the Rand study reveals the major reason why there are such variations in medical practice in the United States: doctors frequently do not agree on what should be done and there is often no objective, "right" answer. Indeed, when the Rand researchers went to great lengths to get consensus, a panel of experts was able to agree on a procedure's appropriateness less than half the time. [91] Medicine, it seems, is often more art than science.
Interestingly, the panel did agree that 12 percent of the time certain procedures were clearly inappropriate. But the cases studied were in the early 1980s, and undoubtedly less inappropriate medicine is practiced today. The reason is that the United States has devoted considerable resources to monitoring the behavior of physicians to high-quality care. Most countries with national health insurance have done little along these lines. [92]
The administrative costs of any production system can be reduced by firing all of the administrators and abolishing all reporting requirements. But most systems would perform far less efficiently as a result. The real goal is not to get administrative costs as low as possible, but to make the system as a whole perform as efficiently as possible.
A similar observation holds for marketing and other costs of competition. Money could be saved by, for example, abolishing all car dealerships and all advertising by auto producers. Money could also be saved by producing a single model car and eliminating competition among different models and different producers. We could simply pay taxes and have government provide us with a new automobile every few years. But the end result would be decreased efficiency and less consumer satisfaction, however. If socialism worked, the economies of communist countries would not have collapsed.
A number of studies have claimed to show that the administrative costs of the Canadian system are well below those in the United States. [93] One problem with these studies is that government accounting techniques invariably underestimate the real cost of government provision of goods and services. [94] A more basic problem is that the studies look only at one aspect of administration (e.g., administrative salaries, costs of paperwork, etc.) while ignoring the effects of administration (e.g., how efficiently the health care system meets consumer needs).
The costs of rationing by waiting and the waste of resources caused by perverse incentives are costs of administering the Canadian system. One cannot legitimately calculate administrative savings in the system without including the adverse effects on patients.
Moreover, many administrative costs in the U.S. system exist not merely to oversee the exchange of money between suppliers and third-party payers. but also to prevent inappropriate care and maintain quality. Even if the United States adopted a program of national health insurance, it is unlikely that we would follow the Canadian practice of giving hospitals global budgets and forcing physicians to ration care with few questions asked.
How the U.S. Tax System Encourages High Administrative Costs.
The administrative costs and paperwork burdens of our system are much too high. That is a consequence not of private provision of health care but of federal policy. Under our tax system, employees (through their employers) can spend unlimited amounts on third-party health insurance. At the same time, any funds employees set aside as selfinsurance for small medical bills face a 15, 28, or 33 percent income tax, a 15.3 percent FICA tax and, usually, a 4, 5, or 6 percent state and local income tax. [95]
As a result of federal tax policies, most employees are overinsured – using third parties to pay for routine checkups, diagnostic tests and other small medical bills. Not only does too much insurance encourage people to be wasteful consumers in the medical marketplace, it also adds to administrative costs:
Studies show that
physicians spend about $8 to process a single insurance claim.
[96]
Most third-party
payers spend another $8 for every check they write, and if the insurer makes an
additional effort to verify the claim, the costs can be much higher.
Thus, a $25
physician's fee can easily become $50 of total costs when third-party payment is
involved – effectively doubling the cost of health care.
Reducing Administrative Costs With Medical Savings Accounts.
A different approach is used in Singapore, where people are required to deposit 6 percent of their salaries each year in personal medical savings accounts, called Medisave accounts. When Singapore residents are hospitalized. they pay the bills from their Medisave funds and avoid many of the administrative burdens of health insurance. [97]
If the U.S. government gave as much tax encouragement to self-insurance through Medisave accounts as it now gives to third-party insurance for the employers and employees of large companies, the administrative costs of U.S. health care could be cut in half.
Whereas the
administrative costs of private health insurance average about 11 to 12 percent
of premiums, payment of medical bills with Medisave funds could be accomplished
by use of health care debit cards – with administrative costs between 1 and 2
percent.
There is no economic
reason why we could not move to a system in which most medical bills are paid by
patients with health care debit cards, relying on third-party insurance to pay
only catastrophic expenses.
[98]
Health Care Debit Cards.
A general system of Medisave accounts would lead naturally to the use of health care debit cards. Patients could, for example, pay for physician visits by using their cards just as people now pay for merchandise at retail stores. Several health care debit card companies already exist, including Pulse Card, headquartered in Kansas City. Kansas, and Security Plus, headquartered in Newport Beach, California. [99]
Health care debit cards could be combined with another technological innovation to reduce other costs and improve the quality of care. Several companies are experimenting with technology that would put a patient's entire medical record on a credit card. [100] This would allow physicians immediate access to each patient's complete medical history. Putting medical records on a credit card could be costly. But it might be less costly than the current system under which physicians treat patients about one-third of the time without access to their records. [101]
The Benefits of the Canadian System Without the Costs.
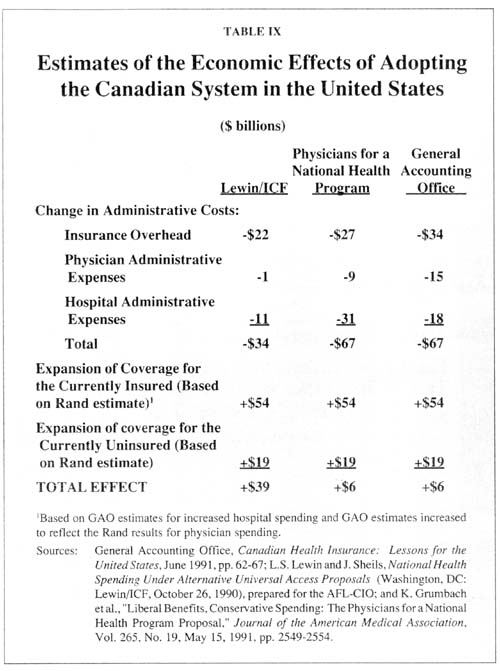
Advocates of the Canadian system of national health insurance cite two principal benefits: 1) patients entering the health care system need produce only a national health insurance card in order to receive care, and 2) the administrative costs of the system are lower because the paperwork is reduced and other costs – such as marketing – are eliminated. Fortunately, the United States can enjoy these advantages without the disadvantages of the Canadian system.
Table IX shows three estimates of how much U.S. administrative costs could be reduced by adopting the Canadian system. The estimates range from a Lewin/ICF estimate of $34 billion to a General Accounting Office (GAO) estimate of $67 billion. As noted above, we believe these estimates are too high.[102] But they may serve as an indicator of potential administrative savings – to the degree medical bills are paid with health care debit cards.
Table IX also shows the additional cost in the United States of making health care absolutely free at the point of consumption as it is in Canada. The estimates are based on the GAO's interpretation of a Rand Corporation study, which found that making medical care free greatly increases the amount consumed – even though the additional consumption has little impact on the patients' health. As the table shows, the additional cost of making health care free for everyone more than offsets even the most optimistic estimate of administrative savings.
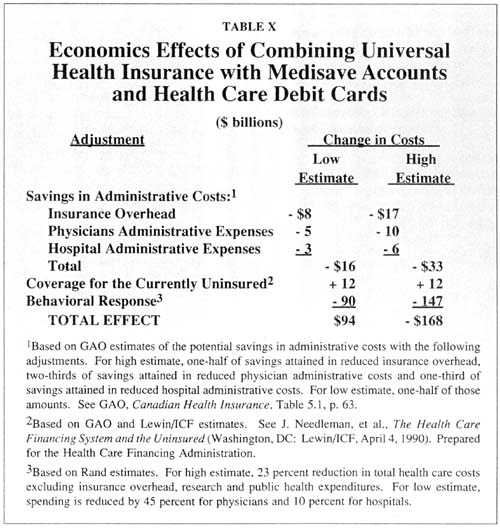
We used the GAO method to estimate the potential reduction in administrative costs under a system of Medisave accounts and health care debit cards, and the Rand Corporation's method to estimate the likely reduction in health care spending if people had high-deductible health insurance. Table X shows the probable effects of a generalized system under which everyone (including Medicaid and Medicare patients) has third-party catastrophic insurance and uses health care debit cards to draw on individual Medisave accounts for small medical bills. As the table shows:
The widespread use of
Medisave accounts would reduce administrative costs by as much as $33 billion.
Because high
deductibles would make patients more prudent purchasers of health care, total
spending would go down by as much as $147 billion.
Overall, universal
catastrophic health insurance combined with Medisave accounts would reduce total
spending by $168 billion – almost one-fourth of what the United States currently
spends on health care.
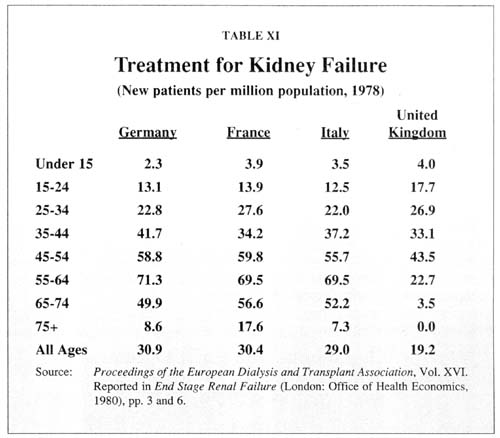
If the experience of other countries is any guide, the elderly have the most to lose. In general, when lifesaving care is rationed, the young get preferential treatment. Take chronic kidney failure, for example. [103]
Across Europe, 22 percent of the dialysis centers reported that they refused to
treat patients over 55 years of age in the late 1970s.
In Britain, 35 percent of the dialysis centers refused to treat patients over
the age of 55, 45 percent refused to treat those over 65 and those over 75 only
rarely received treatment.
Table XI, which shows treatment rates by age for four European countries, illustrates two pertinent features of nonprice rationing of medical care. First, when resources are limited, middle-aged patients get priority over older patients. In Germany, France and Italy, the treatment rates were highest among those aged 55 to 64. In Britain, the treatment rates were highest among those aged 45 to 54. Since our kidneys do not get better with age, these treatment rates undoubtedly reflect rationing decisions rather than medical need.
Second, the more limited the resources, the worse the degree of discrimination against the elderly. For example, for the population as a whole the treatment rates in Germany, France and Italy were 50 percent higher than in Britain. As a result, elderly patients in the first three countries had a much better chance of getting treatment.
These observations are also consistent with more recent evidence on access to heart surgery: [104]
Per capita, the United
States performs twice as many coronary bypass operations on elderly patients as
Canada does.
Among 75-year-olds,
however, the difference between the two countries is four to one.
How serious is the problem of the denial of lifesaving medical technology to elderly patients? Lacking hard data, one can only speculate. In general, health economists arereluctant to take population mortality rates as an indicator of health care quality. This is because whether a person lives or dies in any given year is far more likely to be determined by that person's lifestyle and environment than by anything hospitals or doctors do. In the United States, for example, some people believe that as many as 75 percent of all deaths are directly related to lifestyle. [105]
Despite these caveats, if the life expectancy of any population group is significantly affected by the health care system, it is likely to be the elderly. And international statistics on population mortality are consistent with the proposition that the elderly have the most to lose by nonprice rationing of medical care.
If nonprice rationing results in discrimination against the elderly, then they ought to do better in those countries which spend more on health care – and thus have less of a rationing problem. In order to test this proposition, one recent study compared life expectancy at age 80 among OECD countries. The study found that: [106]
For life expectancy for 80-year-old males, the United States ranked second
(behind Iceland) along with Canada, Japan and Switzerland.
For life expectancy for 80-year-old females, the
United States was second, after Iceland and Canada.
Compared with all OECD countries, an 80-year-old male can expect to live a
half-year longer in the United States, and an 80-year-old female can expect to
live almost a year longer.
There is very little relationship between health care spending and life
expectancy at birth, which tends to correlate with per capita GDP.
However, among 80-year-olds, there is a statistically significant correlation
between life expectancy and health care spending – on a par with the influence
of GDP.
Critics of the U.S. health care system often point to the disadvantages faced by minorities. On the average, African-Americans and Hispanic-Americans are less likely to have health insurance, see a physician or enter a hospital. But is national health insurance the answer?
Both economic theory and empirical studies show that minorities fare worse under systems of nonprice rationing than they do in a marketplace where prices allocate resources. [107] What little evidence we have about health care rationing in the United States is consistent with experience in other fields.
Take the rationing of organ transplants, for example. According to the United Network for Organ Sharing, whites received 97.6 percent of the pancreases and high percentages of livers, kidneys and hearts in 1988. [108] The Pittsburgh Press found that where the donors were not living relatives, the average wait for a kidney transplant in 1988 and 1989 was 14 months for black patients and only 8.8 months for whites. [109] Note that in addition to race, income also matters. A study done by the Urban Institute found that for black and white males, the higher their income the more likely they are to receive an organ transplant. [110]
There have been very few studies of how racial minorities fare under national health insurance in other countries. In a recent study of the Inuits and Crees of northern Quebec, both groups had much less access to health care than Caucasians in southern Quebec and in other areas of Canada – despite their much greater health needs. For example: [111]
The age-adjusted mortality rate for the
Inuit is almost twice the rate for Canada as a whole.
Infant mortality rates are three times greater than for the rest of Quebec among the Cree and four times greater among the Inuits.
Life expectancy at birth in 1978 was only 58.9 years for Inuit males (compared to a Canadian average of 72 years) and 61.6 years for Inuit females (compared to a Canadian average of 79 years). [112]
About 45 percent of the aboriginal people of Ontario live in the rural, northern part of the state. And, as in the case of Quebec, the northern counties are underserved: [113]
In 1986, there were no specialists in allergies and immunology, geriatrics,
infectious diseases and pediatric surgery in all of northern Ontario.
There was only one specialist in dermatology, endocrinology, nephrology,
neurology and rheumatology.
When national health insurance was adopted in 1969, Ontario also adopted a program to encourage physicians to move to rural areas – one of the longest running programs of its kind in the world. Yet a recent study concluded that "while some change has been made, northern Ontario is as underserviced compared to the rest of the province as it was in 1956. " [114]
New Zealand also has both a significant minority population (the Maori) and a comprehensive system of socialized medicine. One study reported that: [115]
New Zealand's Maoris have an infant mortality rate 60 percent higher than
non-Maoris.
Life expectancy for Maori males and females is,
respectively, 7 and 8 years lower than for other New Zealanders.
Only 20 percent of these differences could be explained in terms of
socioeconomic factors.
There is also evidence that the Maoris get significantly less health care – especially in relationship to the need for it – than other New Zealanders. For example:[116]
Death from coronary artery diseases is significantly
higher among the Maori – 3.5 times as high, for example, among females age 25 to
44.
Yet Maoris receive only a tiny fraction of the coronary artery bypass operations
– well below their percentage of the population.
Little is known about who gets care and who does not under nonprice rationing schemes. Britain is one of the few countries that even publishes hospital waiting lists by region and for the country as a whole. Yet in England, as in other countries with national health insurance, rationing decisions are made by doctors and hospital personnel at the local level, and there is no national procedure to guarantee that those in greater need move to the front of the waiting lines.
A study of Norway's health care system concluded that regional differences in waiting times constitute the most serious inequity in accessto health care – more serious, for example, than the distribution of physicians or hospital beds.[117] What is true of Norway is probably also true of other developed countries. For example:[118]
The number of British kidney patients receiving dialysis or a transplant in 1989
averaged 305 people per million population in the four metropolitan areas in and
around London.
The number was only 239 in the northern region of Yorkshire and 174 in the
western region of West Midlands.
These differences are greater than the regional differences in health care spending per person or other measures of health inputs.
There are many reasons to believe that rural patients are at a disadvantage when health care is rationed. [119] The most serious form of rationing is rationing of access to modern medical technology. Often this technology is available only at major hospitals in large cities. This need not be a problem if rural patients can purchase care with their own money or through public or private health insurance. Rationing by waiting, on the other hand, discriminates against rural patients.
For one thing, it often means that care is given to patients who are available when an opening appears in the surgery schedule. Urban patients who live close by thus have an advantage over rural patients who may have to travel considerable distances, requiring both time and inconvenience.
For another thing, success in obtaining care often depends on the politics of bureaucracy. A patient who is represented by a physician in a rural area will tend to be at a disadvantage vis-a-vis a patient represented by a physician who lives nearby and is a colleague of the hospital staff. Urban patients also have access to political and personal relationships that may be important in dealing with bureaucratic obstacles – opportunities not generally available to rural patients.
Finally, wherever there is non-price rationing, people will attempt to move to the head of the waiting lines by paying illegal bribes. In Hungary, the practice of "tipping" has become institutionalized, and each year physicians receive tips equal to about 40 percent of their official total income.[120] In Japan an illegal "gift" of $1,000 to $3,000 can get a patient admitted sooner and insure treatment by a senior specialist at a Tokyo University hospital. [121] In most countries, rural residents probably know less about the mechanics of currying physicians' favors.
Rural Patients in Britain.
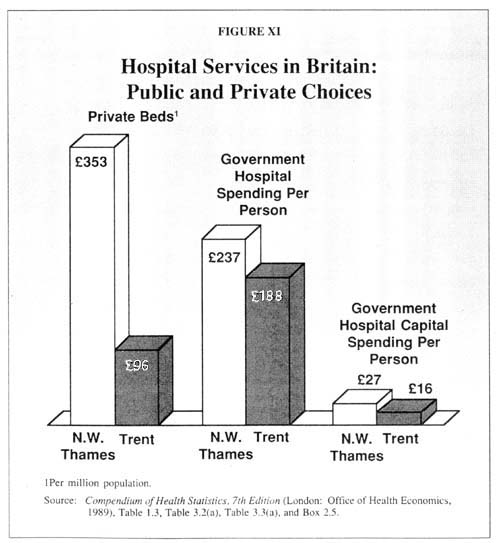
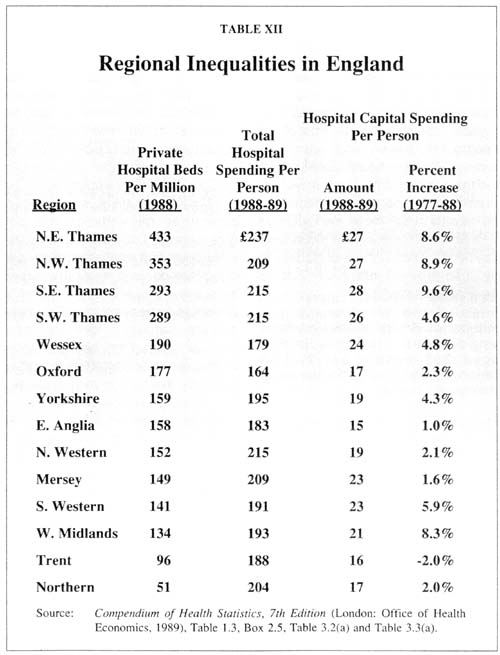
The most important philosophical principle advocated by those who established the British National Health Service was equal access to health care. Yet as we noted above, inequalities across England persist and may even have grown worse since the NHS was founded in 1948. For example, the North East Thames region (near London) has 27 percent more doctors and dentists per person, 15 percent more hospital beds and 12 percent more total health spending than the Trent region (in the more rural northern part of the country). These inequalities do not reflect differences in need. Northerners die younger and are less healthy than southerners.[122]
One way to appreciate the magnitude of these inequalities is to consider them in relation to the growing private health care sector. If the goal of the NHS is to equalize access, one would expect the service to devote more resources to those areas well served by the private sector. In fact, the British government tends to spend the most in the metropolitan areas where private sector alternatives are most abundant.
Table XII lists the regions of England by the number of private beds available per person. Although the correllation is not perfect, in general the more private beds a region has, the greater its odds of also enjoying above-average public hospital spending. For example, as Figure XI shows:
The North East Thames region, which has the largest number of private beds per
person, also enjoys the greatest amount of NHS hospital spending, the second
highest amount of NHS capital spending and the third highest growth in NHS
capital spending over the past decade.
The Northern region – which has the least private hospital beds per person – has
only average NHS hospital spending, the second lowest NHS capital spending and
the fourth lowest growth in capital spending.
The Trent region – which has the second lowest number of private
beds per person – has the second lowest NHS hospital spending per person and the
very lowest NHS capital spending per person, and is the only region that
experienced a decrease in capital spending over the past decade.
Rural Patients in Canada.
Canada, too, has proclaimed equal access to health care a national goal. Yet there is little evidence of success in achieving it: [123]
Among Canadian provinces, the number of people per physician varies from a low
of 471 in British Columbia to a high of 1,273 in the Northwest
Territories – a difference of almost three to one.
Although there are 469 people per physician in Ontario on the average, there are
more than four times that number in each of northern Ontario's rural counties.
As noted above, health care in Canada tends to be hospital-based, with modern technology restricted to teaching hospitals and outpatient surgery discouraged. Moreover, specialists and major hospitals tend to be in major cities. As in other countries, rural residents often travel to the larger cities for medical care. How often does that happen? A major new study produced at the University of British Columbia provides the answer. [124]
Since doctors are paid on a fee-for-service basis in Canada, fee-for-service income is a good measure of the value of services actually rendered to patients. By using physician billing data, Canadian researchers determined the regional hospital district in which each patient lived – even if the service was provided in some other district. As Table XIII and Figure XII show:
Overall, people living
in British Columbia's two largest cities (Vancouver and Victoria) receive about
37 percent more physician services per capita than those living in the 28 rural
districts of the province.
Urban residents
receive 55 percent more services from specialists per capita than rural
residents, and for specific specialties the discrepancies are even greater.
On the average, urban residents are 5-1/2 times more
likely to receive services from a thoracic surgeon, 3-1/2 times more likely to
receive the services of a psychiatrist and about 2-1/2 times more likely to
receive services from a dermatologist, an anesthesiologist or a plastic surgeon.
These are broad averages. The discrepancies are even worse between urban areas and British Columbia's most underserved areas. Table XIV, for example, compares urban spending with spending in 12 other districts for selected services. As the table shows, even if we ignore the smallest districts and focus only on districts with at least 35,000 people, spending varies by a factor of almost 3 to 1 for all specialist services, almost 4 to 1 for OB/GYN services, 8 to 1 for internists and 35 to 1 for psychiatrists.
The discrepancies are greater still among people in specific age and sex classifications in the regions, again ignoring the areas with the smallest populations. Roughly speaking: [125]
An 80-year-old man in
Vancouver is 524 times more likely to receive the services of an
anesthesiologist than if the same man were living in the Sunshine Coast district
(pop. 17,049).
A small child with a
skin rash is 22 times more likely to see a dermatologist if the child is living
in Vancouver than in the East Kootenay district (pop. 50,660).
A baby girl is 10
times more likely to see a pediatrician for any reason if she is living in
Vancouver rather than Peace River (pop. 51,252).
A 40-year-old woman is
almost nine times as likely to have plastic surgery if she is living in
Vancouver rather than Bulkley-Nechako (pop. 36,952).
A 40-year-old woman
with a mental disorder is 12 times more likely to see a psychiatrist if she is
living in Vancouver rather than Fraser-Fort George (pop. 88,250).
Rural Patients in Latin America.
Although this study is focused primarily on developed countries, it is worth noting that many of the same principles apply to people living in less-developed countries. For example, people in urban areas of Brazil are far more successful in getting government benefits than are those in rural areas. By most measures, the need for health care is greater in the north/northeast (rural) areas than in the south/central (urban) areas. Life expectancy at birth, for example, is about three years longer for both men and women in the cities. Yet although most health care spending flows through government and several government programs were designed to create equal access to care, the spending is concentrated in the cities. About one-third of the population lacks regular access to medical care:[126]
Although more than half of Brazil's
population lives in rural areas, residents of urban areas experience nine times
more medical visits, 15 times more related services, 2.7 times more dental
visits and 4.5 times more hospitalizations.
Overall, the Brazilian
government spends five times less on in-patient care and 13 times less on
outpatient care in rural areas.
Brazil is not unique. In neighboring Venezuela, government-provided health care is theoretically free to everyone.[127] Yet the vast majority of health care services are provided in the cities.[128] Similarly, a doctor in Bolivia is seven times more likely to practice in an urban area (where less than half the population resides) than in the countryside.[129] And in Mexico – where health care is a constitutional right – 35 percent of the population (mainly in the cities) consumes 85 percent of the country's health care resources.[130]
Rural Patients in Communist Countries.
It is worth noting that many of the same principles apply to nondemocratic countries. Within communist or formerly communist countries, the variation in rural/urban characteristics is enormous. Throughout the former Soviet Union and Eastern Europe, for example, inequality between urban and rural health care is widespread. In general, the urban populations are healthier and have better access to health care. In the old Soviet Union, health care resources appear to matter a great deal. Indeed, the availability of doctors, nurses and hospital beds explains 55 percent of the variation in infant mortality there. For Bulgaria, Czechoslovakia, Hungary and Poland, the relationships between health care resources and health outcomes are less clear. [131]
Despite the fact that the Soviet Union was committed to the principle of equal access to health care for over 70 years, there is evidence that inequality in access to medical resources and health outcomes grew. [132]
In the 1960s, infant mortality rates were virtually the same, on the average,
among urban and rural areas.
In the 1970s and 1980s, infant mortality rates continued to fall in the cities
but began to rise in rural areas.
Between 1960 and 1987, life expectancy at birth fell so much in rural areas
that by 1986-87 there was a two-year differential in life expectancy between
urban and rural areas.
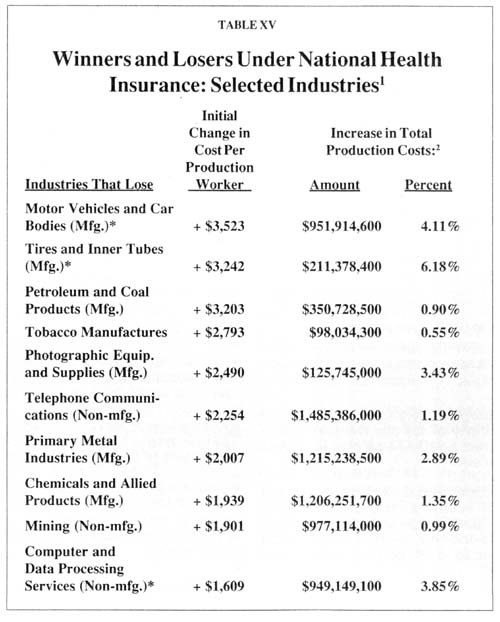
Many leaders of America's largest labor unions advocate national health insurance, believing that they can turn over employee health care costs to the taxpayer. What they forget is that union members also pay taxes. Under national health insurance, the employees of the nation's largest companies would pay more in national health insurance taxes than they currently pay for private health insurance. For example, in manufacturing they would pay 50 percent more. [133]
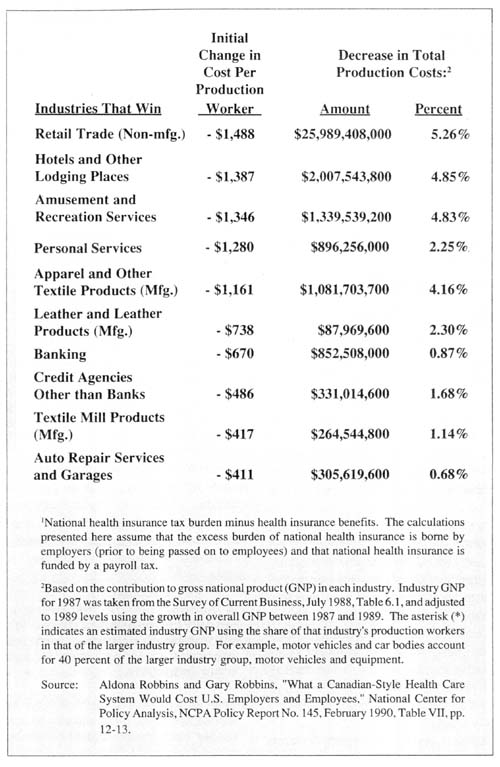
A national health insurance program similar to Canada's would require at least $339 billion in new taxes: [134]
If the program were
funded by a payroll tax, the payroll tax rate would rise from its current level
of 15 percent to at least 30 percent.
If it were funded by an income tax, the current income
tax rate would increase by 16 percentage points, pushing a middle-income worker
from a 28 percent to a 44 percent income tax bracket.
If it were funded by a
consumption tax, the price of everything we buy would increase by almost 10
percent, relative to our income.
These are the tax rates needed to pay for national health insurance for workers and their families. If new health benefits were created for the elderly or for low-income people now covered by Medicaid, tax rates would be even higher. These estimates also assume health care costs remain at their current level. Any rise in health care spending – which is virtually inevitable – would require even more tax revenue.
Note that under each of the broad-based taxes above, the amount paid rises with income. Thus, under national health insurance, the high-wage industries would pay above-average taxes, even though the workers would receive the average benefit. For example : [135]
On the average, the
auto industry would pay about $5,641 per employee under a national health
insurance payroll tax.
Add the loss of the
current deduction for private health insurance and the total cost rises to
$6,824 per auto worker.
Since the industry now
pays only $3,055 for private health insurance, under national health insurance
the cost of health care for auto workers would more than double.
Those industries with below-average wages would pay below-average national health insurance taxes and would experience a financial gain under national health insurance. (See Table XV.) Ironically, some of the latter industries are in the distribution chain of direct competitors to the manufacturing industries. Other things equal, for example, foreign auto dealers would gain a substantial cost advantage over domestic auto producers.
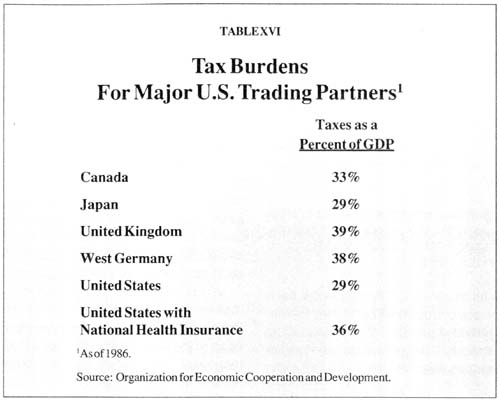
A commonly held view is that U.S. health care costs make U. S. products less competitive in the international marketplace. An example of this view are the assertions that health care costs add $700 to the price of every U.S. automobile and that national health insurance would make American auto manufacturers more competitive. Both assertions are wrong.[136]
There is no evidence whatever that private health insurance costs add anything to the price of an automobile – or of any other product. Health insurance is simply one element in the total compensation package of auto workers, a fringe benefit provided in lieu of money wages. Over the last two decades, fringe benefits for most American workers have grown steadily in real terms, while money wages have grown little, reflecting the preference of employees for nontaxed benefits over taxed wages.
What workers are paid depends on what they produce, not what they consume. The fact that Americans spend a greater proportion of their income on health care and a smaller proportion on other goods and services does not put us at a competitive disadvantage relative to other countries. [137] For example:
The Japanese spend a greater proportion of their income on food, but that
doesn't mean that food consumption adds to the price of a Japanese car.
The Canadians spend a greater proportion of their income on education but that doesn't mean
that education adds to the price of Canadian lumber.
The differences in consumption patterns merely reflect consumer preferences and consumer product prices.
However, national health insurance would affect our ability to compete in international markets. That is because such insurance involves not only the purchase of health care but also a redistribution of income among producers in different industries. On the whole:
A national health
insurance system would impose extra taxes on U.S. exporting industries and use
the proceeds of those taxes to subsidize other industries.
The industries which would receive subsidies
contribute mostly to domestic rather than international markets.
The industries which
would be penalized are the manufacturers which provide most of our exports.
National health insurance would raise the costs of our export goods and lower marketing costs in the U.S. for our foreign competitors. Far from making auto producers more competitive in international markets, it would raise auto production costs relative to foreign rivals and make the industry less competitive.
Despite the fact that one-third of our federal budget goes to defense spending, a burden not equaled by our trading partners, taxes are lower in the U.S. than in most developed countries. As Table XVI shows, only Japan currently has a tax burden as low as ours. Were we to adopt a program of national health insurance, the U.S. tax burden would approach that of Britain and Germany. That additional burden would have a major impact on our ability to compete.
Of all the characteristics of foreign health care systems, the one that strikes American observers as the most bizarre is the way in which limited resources are allocated among competing needs. Foreign governments do not merely deny lifesaving medical technology to patients under national insurance schemes.
They also take millions of dollars that could be spent to save lives and cure diseases, and spend them to provide services to people who are not seriously ill. Often, these services have little if anything to do with health care.
Britain, once again, exemplifies this behavior. Throughout the National HealthService, there is a pervasive tendency to divert funds from expensive care for the small number who are seriously ill toward the large number who seek relatively inexpensive services for minor ills. Take the British ambulance service, for example: [138]
English "patients" take more than 2l million ambulance rides each year – about
one ride for every two people in England.
About 91 percent of these rides are for nonemergency purposes (such as taking an
elderly person to a local pharmacy) and amount to what an official task force
report described as little more than "free taxi service."
Yet for genuine emergencies, the typical British ambulance lacks the modern,
lifesaving equipment considered standard in American cities.
While as many as 9,000 people die each year from lack of treatment for kidney failure, the NHS provides an array of comforts for the many chronically ill people whose kidneys are in good working order:
Each year about 4.1 million people in England are treated in their homes by
"health visitors " – more than 1.1 million are treated in their homes by
chiropodists and "meals on wheels" serves almost 33 million meals in people's
homes.
Social workers attending to the needs of the elderly and the handicapped help
with the installation of more than 17,000 telephones and telephone attachments,
help arrange more than 93,000 telephone rentals, help more than 49,000 people
with home alterations, assist in arrangements for 63,000 vacations and help an
additional 346,000 people with other personal appliances and aids.
While tens of thousands of people classified by their physicians as being in "urgent need" of surgery wait for hospital beds, the NHS spends millions on items that have only marginal effects on health:
On the average, the NHS spends more than $90 million each year on tranquilizers,
sedatives and sleeping pills, almost $32 million on antacids and about $11
million on cough medicine.
About 9.7 million people receive "free" eyesight tests every year, and of these
about 2.3 million receive free or subsidized eyeglasses.
[139]
If the NHS did nothing more than charge patients the full costs of their sleeping pills and tranquilizers, enough money would be freed to treat 10,000 to 15,000 additional cancer patients each year and save the lives of an additional 3,000 kidney patients. Yet such options are not seriously considered.
A full description of the ways in which "caring" takes priority over "curing" within the British National Health Service would fill a volume the size of a phone book, and readers may wish to consult other references. [140] Suffice it here to say that the tendency pervades every aspect of British medicine.
Spending Priorities in Canada.
Although not as pronounced, similar trends can be observed in Canada, where the government has expanded the services of general practitioners while tightly controlling access to modern medical technology. For example: [141]
In the United States, only 13 percent of all
physicians are engaged in general practice or family practice.
In Canada, over half of all physicians are general practitioners and the
percentage of GPs has been rising over the past two decades.
Ontario even has a
policy requiring that 55 percent of its physicians be in general practice.
In general, Canadians have little trouble seeing a GP. But specialist services and sophisticated equipment are increasingly rationed. As noted above, although the United States has seen a major expansion of outpatient surgery, Canada has actively discouraged this trend – presumably to control spending. All over Canada, CAT scanners and other equipment are restricted to hospitals, and Ontario has legislated this restriction.[142] The Canadian system encourages the provision of routine services for the many at the expense of specialized care for the few. As one Canadian economist observed, "A growing number of operations are triaged because resources are used to continue first-dollar coverage for sniffles and splinters." [143]
A common argument for national health insurance is that "free" health care saves money by encouraging preventive services, which allow doctors to catch conditions in their early stages – before they develop into more costly-to-treat diseases. The argument is wrong for two reasons.
First, careful studies show that, in general, preventive medicine raises rather than lowers overall health care costs. Preventive medicine is "economical" only when special at-risk groups are targeted. Giving preventive services to the entire population usually costs more than any savings from early detection of disease. [144] This does not mean that preventive care is undesirable. Diagnostic tests which show that no disease is present benefit patients – relieving anxiety and creating reassurance of health. Preventive care is like a consumer good which creates benefits in return for a cost. It is not like an investment good which promises a positive economic rate of return.
Second, under national health insurance preventive care may actually become less available, precisely because care is free. A comparison of American and British GPs in the 1970s found that the British saw a GP four times as often. Yet when Americans did see a doctor, they spent two-and-one-halftimes as long with the physician and received far more preventive services. [145]
Because the services of GPs are "free" to Britons, an inordinate number of their visits are for trivial complaints. In order to handle the case load, British doctors have responded by spending less time with each patient. Moreover, because of the British government's desire to control costs, British physicians have much less access to diagnostic equipment, and most send their patients to a hospital even for chest x-rays and simple blood tests. As a result, preventive medical care is slighted in the NHS system. According to the 1970s comparison: "Even though GPs receive an extra fee for cervical cytology tests (PAP smears), most will not provide such tests unless patients insist. The attitude is similar for breast checks. In 1976, only 8 percent of eligible females received PAP smears, and most of these were given to middle and upper-middle class patients. (By contrast, in 1973 almost 46 percent of American women age 17 or older had been given a PAP test within the previous 12 months.) GPs also receive extra payments for certain kinds of vaccinations. But again, it appears that the inducement is small. Over the last decade there has been a general decline in the percentage of children vaccinated against every major childhood disease." [146]
One consequence of the lack of preventive care in Britain is that many illnesses are never diagnosed. For example, a series of screenings conducted by the British government several decades ago implied that for every case of diabetes, rheumatism or epilepsy known to a general practitioner, another was undiagnosed. For every case of psychiatric illness, bronchitis, blood pressure, glaucoma and urinary infection, another five were undiagnosed. For every known case of anemia, eight were undiagnosed. [147] The evidence suggests that things may not have improved: [148]
A fairly recent study
(1989) concluded that for every diabetic being treated under the National Health Service,
another case of diabetes is undiagnosed.
Another study (1988)
suggests that one in 20 diabetics in England is first diagnosed by an
optometrist (when the disease is in its late stages), who then refers the
patient to a general practitioner.
At one-half the age of the British system, Canadian national health insurance does a better job – but suffers from similar problems. Although Canadians see their physicians more often than Americans do, a Canadian is not entitled to a routine cholesterol check, unless some other condition warrants it. [149] And we have already seen how limits on technology have caused extensive waits for other diagnostic services, including PAP smears, mammograms and CAT scans.
Note that the United States does not necessarily do a better job at delivering preventive medicine. As in the case of Britain, it is believed that one out of every two U.S. diabetics is undiagnosed and one recent study reported that between 1980 and 1986, there were 121,560 deaths from disorders that are usually not lethal if discovered and treated early. [150] However, as the discussion above shows, socializing the health care system by no means guarantees that these problems will be solved.
The characteristics described above are not accidental by-products of government-run health care systems. They are the natural and inevitable consequences of politicizing medical practice.
Why are low-income and elderly patients so frequently discriminated against under national health insurance? Because such insurance is always and everywhere a middle-class phenomenon. Prior to its introduction, every country had some government-funded program to meet the health care needs of the poor. The middle-class working population not only paid for its own health care but also paid taxes to fund health care for the poor. National health insurance extends the "free ride" to those who pay taxes to support it. Such systems respond to the political demands of the middle-class working population, and they serve the interests of this population.
Why do national health insurance schemes skimp on expensive services to the seriously ill while providing so many inexpensive services to those who are only marginally ill? Because the latter services benefit millions of people (read: millions of voters), while acute and intensive care services concentrate large amounts of money on a handful of patients (read: small number of voters). Democratic political pressures in this case dictate the redistribution of resources from the few to the many.
Why are sensitive rationing decisions and other issues of hospital management left to hospital bureaucracies? Because the alternative is politically impossible. As a practical matter, no government can make it a national policy that 9,000 people will die every year because they will be denied treatment for chronic kidney failure. Nor can any government announce that some people must wait for surgery so that the elderly can use hospitals as nursing homes, or that elderly patients must be moved so that surgery can proceed.
These decisions are so emotionally loaded that no elected official can afford to claim responsibility for them. Important decisions on who will and will not receive care and on haw that care will be delivered are left to the hospital bureaucracy because no other course is politically possible.
As far back as the presidency of Richard Nixon, polls showed as much as 61 percent of the people favored national health insurance. [151] And only 3 percent of Canadians and12 percent of the British say they would trade their own system for the U.S. health care system. [152] But on closer examination, all those polls tell us is that most people prefer a free lunch.
Polls also tell us that most Britons believe the cost to them of national health insurance is about 1/20th of what it actually costs. At 1/20th of its real costs, the British health care system might look attractive to most people. Since health care taxes are also disguised in Canada, it seems likely that Canadians are unaware of their individual contribution to national health insurance as well. Thus, most of these people think they get a lot more than they pay for. And given the international publicity about the American health care costs, it's not surprising that people prefer something-for-nothing rather than something better but very expensive.
When individuals are asked to compare benefits with costs, their responses to polls are much more revealing. Roughly speaking, people prefer to see government spend more on health care, provided their own taxes are not increased to finance the spending. For example:
By a margin of 71 to
26 percent, Americans agree that, "Health insurance should pay for any treatments that
will save lives even if it costs one million dollars to save a life."
When the
United States was spending 8.2 percent of GNP on health care, most respondents
thought we were spending 13 to 15 percent and identified 16 to 20 percent as the
appropriate amount.[153]
A majority favor
covering the uninsured through employer mandates or through an expansion of
Medicare.[154]
But when asked about
paying, people were unwilling to pay higher income taxes and supported the
proposal only if it were financed by "sin taxes" or taxes on employers.
[155]
Thus, polling data give no indication that people are willing to pay 15 percent of their income to finance national health insurance. Nor do the polls indicate that Americans are willing to accept the negative aspects of national health insurance. For example: [156]
The public
overwhelmingly disapproves of any cost-containment measure that translates into
a lower quality of care.
By a margin of 81 to
18 percent, the public is unwilling to accept longer waits for doctor's
appointments or elective surgery.
National health insurance "works" in other countries for three reasons. First, the wealthy, powerful and sophisticated – those most skilled at articulating their complaints – find ways to maneuver to the front of the rationing lines. Second, those pushed to the end of the lines are generally unaware of medical technologies they are being denied. Third, there are no (or severely limited) contingency fees, no generally recognized right of due process and no cadre of lawyers willing to represent those who are discriminated against.
National health insurance "works" in other countries because those who could change the system are best served by it. If a member of the British Parliament, the CEO of a large British company or the head of a major British trade union had no greater access to renal dialysis than any other British citizen, the British NHS would not last a week.
"Don't push me around" is a distinctly American phrase. In the United States we have widespread access to information about modern medical technology, a legal system that protects the rights of those without political power or money, and a strong devotion to basic rights of due process. National health insurance, as it operates in other countries, simply would not survive in the U.S. cultural and legal system.
Chrysler Chairman Lee lacocca, the United Auto Workers and many others have looked longingly at the health care systems of other countries and called for a U.S. government solution. But do the workers at Chrysler really need government in order to adopt the health care programs of other countries? It is not at all clear that they do.
The primary way other developed countries control health care costs is through "global budgets." Hospitals, physicians or area health authorities are told by government how much money they have to spend. The government then leaves decisions about how to ration the funds to the health care bureaucracy. [157]
There is nothing mysterious about this process, and no reason why Chrysler needs government in order to copy it. For example, Chrysler workers or any other large group could form their own HMO, called a national health insurance HMO (NHI HMO). The total amount of money given to NHI HMO each year could be 75 percent or even 50 percent of what Chrysler now spends on employee health care, and the NHI HMO managers could be instructed to ration care to Chrysler workers.
If Chrysler workers wanted to exert more direct control, they could elect the chief executive officer of the NHI HMO in annual balloting, and candidacy could be open to all health care bureaucrats or restricted to those with certain qualifications. The most obvious obstacle Chrysler would face would be U.S. tort law. If NHI HMO physicians rationed medical care the way the British do, there would be many potential malpractice suits. But if Chrysler workers owned their own HMO and if enough legal documents were signed, even this obstacle could be overcome.
In short, Chrysler employees could realize "benefits" of national health insurance through private action, without government intervention, provided that is their sincere objective. On the other hand, if the rhetoric coming from Chrysler is merely a ruse to get taxpayers to pay Chrysler's annual health care bill, federal government coercion would be required.
Our survey of national health insurance in countries around the world provides convincing evidence that government control of health care usually makes citizens worse off. When health care is made free at the point of consumption, rationing by waiting is inevitable. Government control of the health care system makes the rationing problem worse as governments attempt to limit access to modern medical technology. Under government management, both efficiency and quality of patient care steadily deteriorate.
The lesson from other countries is that America would not be well-served by an expansion of government bureaucracy or by greater governmental control over the U.S. health care system. Instead, what is needed is to limit the role of government and allow the private sector to solve our health care problems.
(Editor's Note: Forthcoming studies and commentaries from The Mackinac Center for Public Policy will take up where this report leaves off and suggest numerous public policy reforms to solve the health care crisis – in Michigan and across America – by invigorating the private sector.)
See Patricia Day and Rudolf Klein, "Britain's Health Care Experiment." Health Affairs, Fall 1991, pp. 39-59; and Alain C. Enthoven, "Internal Market Reform of the British Health Service,: Health Affairs, Fall 1991, pp. 60-70.
Jeremy W. Hurst, "Reforming Health Care in Seven European Nations." Health Affairs, Fall 1991, pp. 18-19.
Ibid., p. 18.
A blueprint for the reforms maybe found in Patricia Danzon and Susan Begg, Options For Health Care in New Zealand (Wellington: New Zealand Business Roundtable, 1991).
For general changes in Europe, seethe discussion in Bengt Jonsson, "What Can Americans Learn From Europeans?", Symposium: International Comparisons of Health Care Systems, Health Care Financing Review, Annual Supplement, 1989, pp. 79-93.
See Clyde H. Farnsworth, "Economic Woes Force Canada to Reexamine Medical System," New York Times, November 24, 1991; and Edward Neuschler, Canadian Health Care: The Implications of Public Health Insurance (Washington, DC: Health Insurance Association of America, 1989), p.52.
See Diane Rowland and Alexandre V. Telyrikov, "Soviet Health Care From Two Perspectives, " Health Affair, Fall 1991, pp. 71-86.
For a description of Chile's health care reforms, see John C. Goodman and Peter A. Ferrara, "Private Alternatives to Social Security in Other Countries," National Center for Policy Analysis, NCPA Policy Report No. 132, April 1987; and Tarsicio Castaneda, "The Chilean Health System: Organization, Operation and Financing," in Health Economics: Latin American Perspectives (Washington, CD: Pan American Health Organization, 1989), pp. 3-25.
The regression equation is: HEXP = -5.99 + 1.36 GDP (R = .89) (-5.6) (11.9)
Where HEXP is the logarithm of per capita health care spending, GDP is the logarithm of per capita gross domestic product, and the numbers in parenthesis are t values. The U.S. figure falls near the upper bound of a 95 percent confidence interval. Figures for the higher-income countries, such as Denmark, Luxembourg and Norway fall closer to the lower bound, possibly because of underreporting of certain types of expenditures, such as nursing home care. See Bengt Jonsson, "What Can Americans Learn from Europeans?", p. 83.
The analysis that follows is based on Neuschler, Canadian Health Care, pp. 37-53. For a critique of this approach see Morris L. Barer, W. Pete Welch and Laurie Antioch, "Canadian/U.S. Health Care: Reflections on the H IAA's Analysis," Health Affairs, Fall 1991, pp. 229-236.
Ibid.
Ibid.
Jacques Krasny, The Canadian Health Care System in Perspective (Morristown, NJ: Bogart Delafield Ferrier, Inc., 1989) and Jacques Krasny and Ian R. Ferrier, "A Closer Look at Health Care in Canada," Health Affairs, Summer 1991, pp. 152-158. See, however, a critique of this approach in Daniel R. Waldo and Sally T. Sonnefeld, "U.S./Canadian Health Spending: Methods and Assumptions," Health Affairs, Summer 1991, pp. 159-164.
Leroy L. Schwartz, "The Medical Cost of America's Social Ills," Wall Street Journal, June 24,1991. See also Spencer Rich, "Tracing Medical Costs to Social Problems," Washington Post, August 28,1991.
See the discussion in Neuschler, Canadian Health Care, p. 50.
This section is based on Dale A. Rublee and Markus Schneider, "International Health Spending: Comparisons With the OECD," Health Affairs, Fall 1991, pp. 187-198. See, however, a critique of this approach in George J. Schieber and Jean-Pierre Poullier, "Advancing the Debate on International Spending Comparisons," Health Affairs, Fall 1991, pp. 199-201.
Finn Diderichsen, "Health and Social Inequities in Sweden," Social Science and Medicine, 1990, Vol. 31, No. 3, Table IV, p. 363.
Per Maseide, "Health and Social Inequities in Norway," Social Science and Medicine, Vol. 31, No. 3,1990, pp. 331-342.
Maseide, "Health and Social Inequities in Norway," Table 1, p.333.
Michael Walker (Fraser Institute), "Why Canada's Health Care System Is No Cure for America's Ills," Heritage Foundation Backgrounder, November 13,1989, pp. 7-8.
The treatment for patients with chronic renal failure and the use of CAT scanners continued its rise in virtually every country throughout the 1980s – an acknowledgment of the medical value of these innovations. Some have argued that the U.S. went too far in its use of pacemaker implants, however.
See John C. Goodman, National Health Care in Great Britain (Dallas: Fisher Institute, 1980), pp. 96-104.
Jonsson, "What Can Americans Learn From Europeans?", Table 8, p. 88.
Ibid., pp. 88-89.
lbid., Table 10, p. 89.
See John C. Goodman and Gerald L. Musgrave, Patient Power: Solving America's Health Care Crisis (Washington, DC: Cato Institute, forthcoming).
Day and Klein, "Britain's Health Care Experiment," p. 43. For discussion of British hospital rationing, see Goodman, National Health Care in Great Britain, ch. 6. Enoch Powell, former Minister of Health, has argued that waiting lines are inevitable under the NHS, regardless of the resources devoted to health care. See Enoch Powell, Medicine and Politics, 1975 and After (New York: Pitman, 1976).
For an analysis of the waiting list in New Zealand, see Choices for Health Care: Report of the Health Benefits Review (Wellington: Health Benefits Review Committee, 1986), pp. 78-79.
Estimate of the Fraser Institute (Vancouver) based on sampling in five Canadian Provinces.
Hospital admissions as a percent of the total population average 16.1 percent for all OECD countries. The figures are 15.9 percent for the United Kingdom, 13 percent for New Zealand and 14.5 percent for Canada. See Schieber et al., "Health Systems in Twenty-four Countries," Exhibit 4, p.27.
Health insurance industry officials in the United States report that about 4 percent of the population consumes about 50 percent of health care costs. See Blue Cross/Blue Shield, Reforming the Small Group Health Insurance Market (Chicago: BC/BS, 1991), p. 6.
For example, in Ontario in 1989 the number of people waiting for open-heart surgery equaled more than 25 percent of the total surgeries performed. Because of special efforts to reduce the waiting lists, Ontario achieved a rate of one person waiting for every seven surgeries by January 1991. See C. David Naylor, "A Different View of Queues in Ontario," Health Affairs, Fall 1991, pp. 115116.
Danzon and Begg. Options for Health Care in New Zealand, Table 2-3, p. 26.
General Accounting Office, Canadian Health Insurance: Lessons for the United States, June 1991, Table 4. 1, p. 55.
See, for example, Joan Breckenridge, "Grief, Frustration Left in Wake Of Man Who Died on Waiting List," Globe and Mail (Ontario), January 25, 1989.
For Britain, see the discussion in Enthoven, "Internal Market Reform of the British Health Service." A Canadian observer reports that "Ontario hospitals lag at least a decade behind their U. S. counterparts in expenditure tracking and management information systems. "See Naylor, "A Different View of Queues in Ontario, "p.112.
Enthoven, "Internal Market Reform of the British Health Service," p. 62
For New Zealand, estimate of the New Zealand Department of Health. OECD Statistics show an occupancy rate of 74.8 percent for New Zealand in 1983 and 83.3 percent for Canada. See Organization for Economic Cooperation and Development, Financing and Delivering Health Care (Paris: OECD, 1987), Table 29, p. 67. The most recent OECD statistics are expected to show an occupancy rate of 80.3 percent for acute care hospitals and 82.7 percent for all hospitals in Canada for 1987. See George J. Schieber et al.. "Health Care Systems in Twenty-four Countries," Exhibits 4 and 5, pp. 27.29.
Hospital occupancy rates are 74 percent for acute beds and 82 percent for all beds. See Office of Health Economics, Compendium of Health Statistics: 7th Edition, 1989 (London: OHE, 1989) section 3, p. 39. The most recent OECD statistics are expected to show an occupancy rate of 76.4 percent for acute care hospitals and 80.6 percent for all hospitals in 1986. See Schieber et al.. "Health Care Systems in Twenty-four Countries," Exhibits 4 and 5, pp'. 27, 29.
In Canada, the latest estimate is 23 percent. See Neuschler, Canadian Health Care, p.18.
See Rosie DiManno, "Hard Choices Facing Health Care System," Toronto Star, January 28,1989; "Ceiling System Needs Radical Surgery." (Sunday) Toronto Star, March 27,1988; and Robert G. Evans et al., "Controlling Health Expenditures: The Canadian Reality." New England Journal of Medicine, Vol: 320, No. 9, March 2. 1989, p. 5
For an analysis of international length of stay statistics, see Rita Ricardo-Campbell, The Economics and Politics of Health (Chapel Hill, NC: University of North Carolina Press, 1982), Table 3, p.85: and Cotton M. Lindsay et al., National Health Issues: The British Experience (Nutley, NJ: Hoffmann-LaRoche, Inc., 1980), pp. 74-78.
See the discussion in Schieber et al., "Health Care Systems in Twenty-four Countries," pp. 28-30.
Quoted in Economic Models, Ltd., The British Health Care System (Chicago: American Medical Association, 1976),p.33.
Quoted in Harry Swartz, "The Infirmity of British Medicine," in Emmett Tyrrell, Jr., ed., The Future That Doesn't Work: Social Democracy's Failures in Britain (New York: Doubleday, 1977), p. 24.
British Medical Journal, December 12,1942, p. 700.
Aneurin Bevan, In Place of Fear (London: Heinemann, 1952), p.76.
Inequalities in Health (Black report), (London: Department of Health and Social Security, 1980).
See Julian LeFrand, "The Distribution of Public Expenditure: The Case of Health Care," Economica, Vol. 45, No. 178, 1978: Anthony J. Culyer, Need and the National Health Service (Totowa, NJ: Rowman and Lettlefield, 1976); Michael H. Cooper, Rationing Health Care (New York: Halstead Press, 1975); Michael H. Cooper and Anthony J. Culyer, "Equality in the N.H.S.: Intentions, Performance and Problems in Evaluation," in M. M. Houser, ed., The Economics of Medical Care (London: Allen and Unwin, 1972); J. Noyce, A. A. Snaith and A. J. Trickey, "Regional Variations in the Allocation of Financial Resources to the Community Health Services," The Lancet, March 30,1974; and Goodman, National Health Care in Great Britain, ch. 9. For a recent update on government failures to make any progress in achieving equality of access to health care, see "Dying of Inequality," The Economist, April 4,1987, p. 52.
Noyce, Snaith and Trickey, "Regional Variations in the Allocation of Financial Resources to the Community Health Service," Table III, p. 556.
Julian LeGrand, "The Distribution of Public Expenditure: The Case of Health Care," Economica, Vol. 45, No. 178, May 1978.
See Ingemar Stahl, "Can Equity and Efficiency Be Combined: The Experience of the Planned Swedish Health Care System," in Mancur Olson, ed., A New Approach to the Economics of Health Care (Washington, DC: American Enterprise Institute, 1981), pp. 187-190.
Cotton M. Lindsay, Canadian National Health Insurance: Lessons for the United States (Nutley, NJ: Hoffmann-LaRoche, 1979).
Choices for Health Care, pp. 19-22.
General Office of Accounting, Canadian Health Insurance, pp. 53 ff.
Areview of the hospital records of open-heart surgery patients in Toronto found that while physicians generally assign sensible priorities, there were "many instances of relatively short waits for elective cases while more urgent cases waited inappropriately long periods of time." See Naylor, "A Different View of Queues in Ontario," p.121.
Public Health in the Provinces," p. 14.
Walker, "Why Canada's Health Care System Is No Cure for America's Ills," p. 9.
Robert J. Blendon and Humphrey Taylor, "Views on Health Care: Public Opinion in Three Nations," Health Affairs, Sprint 1989, p.156.
Ibid.
Day and Klein, "Britain's Health Care Experiment," pp. 43-44.
Choices for Health Care, p. 75.
Neuschler, Canadian Health Care, pp. 17-18 and p. 20.
Ibid.
DiManno, "Hard Choices Facing Health Care System."
Tracey Tyler, "Frustrated Heart Patients Head to Ohio For Surgery," Toronto Star, January 22.1989.
Neuschler, Canadian Health Care, p. 50.
Ibid.
John K. Iglehart, "Canada's Health Care System Faces Its Problems," New England Journal of Medicine, Vol 322, No. 8, p. 566.
Milan Korcak, "US Cash Registers Humming as Canadian Patients Flock South," Canadian Medical Association Journal, Vol. 144, No. 6, February 1991, pp. 745-747.
David Caplan, letter to the editor of New England Journal of Medicine (July 13,1989), p.115. Reprinted in the House Wednesday Group, "Public Health in the Provinces," September 22,1989, p.12.
Public Health in the Provinces," p. 14.
"The Crisis in Health Care: Sick to Death," Macleans, February 13, 1989, p. 32.
Walker, "Why Canada's Health Care System is No Cure for America's Ills," p. 9.
"Canadians Cross Border to Save Their Lives," Wall Street Journal, December 12,1990 - Cited in Michael Tanner, "Canadian Health Care in American: Prescription for Disaster," American Legislative Exchange Council, State Factor, Vol. 17, No. 8. June 1991,p.1.
Ottawa Citizen, February 4, 1989. Cited in "Public Health in the Provinces." p. 15.
"The Crisis in Health Care," p. 32.
Ibid.
Ibid.
Ibid., p. 33.
Globe and Mail (Ontario), May 28, 1988. Cited in Neuschler.Canadian Health Care. p.48.e2
Toronto Sun, September 14.1989. Cited in Neushler, Canadian Health Care, p. 93.
Edmonton Journal,January 6, 1990. Cited in Neuschler, Canadian Health Care, p. 96.
Winnipeg Free Press, July 5, 1989. Cited in Neuschler, Canadian Health Care, p. 94.
St. John's Evening Telegram, June 28, 1989. Cited in Neuschler, Canadian Health Care, p. 94.
Canadian Broadcasting Company radio show, "As It Appears," January 25,1989. Cited in Neuschler, Canadian Health Care, p. 95.
Robert H. Brook, "Practice Guidelines and Practicing Medicine: Are They Compatible?", Journal of the American Medical Association, Vol. 262, No. 21, December 1, 1989, p. 3028.
A summary of Rand research may be found in Mark R. Chassin, ed., The Appropriateness of Selected Medical and Surgical Procedures (Ann Arbor; Health Administration Press, 1989).
George Telling Smith, Patterns of Prescribing (London: Office of Health Economics, 1991).
Office of Health Economics, "Variations Between General Practitioners." OHE Briefing, No. 26, July 1990.
Brook, "Practicing Guidelines and Practicing Medicine: Are They Incompatible?", p. 3021.
See, for example, Adam L. Linton, "Guidelines for Medical Practice: The Reasons Why," Canadian Medical Association Journal, Vol. 143, No. 6. pp. 485-490.
For example, one study claimed that administrative costs in the United States were between 19.3 percent and 24.1 percent of total health care spending and accounted for more than half the difference in cost between the U. S. and Canadian systems. See Steffie Woolhandler and David Himmelstein, "The Deteriorating Administrative Efficiency of the U. S. Health Care System," New England Journal of Medicine, Vol. 324, No. 18, May 2,1991, pp. 1253-1258. See also a critique of the study's methodology by the Health Insurance Association of America in Medical Benefits, Vol. 8, No. 10, May 30, 1991, p. 5. In another study, a national health insurance advocacy group, Citizen Fund. claimed that 33.5 cents of every dollar spent by private health insurance was for overhead expenses. See Richard Koenig. "Insurers' Overhead Dwarfs Medicare's," Wall Street Journal, November 15, 1990. The results of other studies are reviewed below.
E. S. Savas. "How Much Do Government Services Really Cost?" Urban Affairs Quarterly, September 1979, p. 24.
See John C. Goodman, Gary Robbins and Aldona Robbins, Employee Benefits Law: The Case for Radical Reform," National Center for Policy Analysis, NC PA Policy Report No. 147, March 1990.
American Medical Association Center for Health Policy Research, "The Administrative Burden of Health Insurance on Physicians," SMS Report, Vol. 3, No. 2. 1989.
See the description in Goodman and Ferrara, "Private Alternatives to Social Security in Other Countries."
See John C. Goodman and Gerald L. Musgrave, "Controlling Health Care Costs With Medical Savings Accounts." National Center for Policy Analysis. forthcoming.
See Burt Sims, "Cutting Health Care Costs: A Major Breakthrough," US Business to Business, Winter 1991.
Currently, there are three competing technologies: magnetic striped cards, smart cards (with integrated circuits) and optical memory ;laser) cards. See C. Peter Waegemann, "Patient Cards – The Promise of the Future?". Medical Practice Management, Spring 1990, pp. 264-268.
Ibid., p. 264.
For critiques of these estimates, see 'GAO Report on Canadian Health Care Tainted by Charges of Partisanship," Health Benefits Letter, Vol. 1, No. 16, September 18, 1991; and the letters to the editor in the New England Journal of Medicine. Vol. 325. No. 18. pp. 1316-1319.
End-Stage Renal Failure (London: Office of Health Economics, 1980), pp. 3 and 6.
See G. M. Anderson, J. P. Newhouse and L. L. Roos, "Hospital Care for Elderly Patients with Diseases of the Circulatory System: A Comparison of Hospital Use in the United States and Canada," New England Journal of Medicine, Vol. 321, 1989, pp. 1443-1448: and the discussion in Naylor, "A Different View of Queues in Ontario," pp. 117-118.
Jack A. Meyer and Marion E. Lewin, "Introduction," in Meyer and Lewin, eds., Charting The Future of Health Care (Washington, DC: American Enterprise Institute. 1987), p.5.
Schieber et al., "Health Care Systems in Twenty-four Countries," pp. 36-37.
See Walter Williams, "Legislating Black Unemployment." National Center for Policy Analysis, NCPA Policy Report No. 112. July 1984.
Associated Press, May 20, 1989.
Reported in the Dallas Morning News, August 19, 1990.
Phillip J. Held, Ph.D. et al., "Access to Kidney Transplantation: Has the United States Eliminated Income and Racial Differences?", Archives of Internal Medicine, Vol. 148, December 1988, pp. 2594-2600. A possible reason for the discrepancy is Medicare reimbursement policies, which place greater burdens on lower-income patients. Prior to 1987 (the period covered by the study), Medicare did not pay for outpatient drugs such as cyclosporine – which can cost transplant patients up to $5,000 per year. It would be irrational to spend $50,000 on a transplant and have it rejected because the patient could not afford $5,000 in medication. Currently, Medicare pays for 80 percent of immunosuppressive drugs for one year.
Jean-Pierre Thorrez, Peter Foggin and Andre Rannou, "Correlates of Health Care Use: Inuit and Cree of Northern Quebec," Social Science and Medicine. Vol. 30, No. 1, pp. 25-34.
Canadian average life expectancy is for 1982.
Malcolm Anderson and Mark W. Rosenberg, "Ontario's Underserviced Area Program Revisited: An Indirect Analysis," Social Science and Medicine, Vol. 30, No. 1, pp. 35-44.
Ibid., p. 43.
E. W. Pomare, "Groups with Special Health Care Needs," New Zealand Medical Journal, October 26, 1988, pp. 711-713.
Ibid.
Maseide, "Health and Social Inequities in Norway," p. 331.
Office of Health Economics. Compendium of Health Statistics, 7th Edition, 1989, Table 3.36(a), p. 49.
See John C. Goodman and Gerald L. Musgrave, "National Health Insurance and Rural Health Care," National Center for Policy Analysis, NCPA Policy Report No. 107, October 1991.
Lajos Csaszi, "Interpreting Inequalities in the Hungarian Health System," Social Science and Medicine, Vol. 31, No. 3, p. 280.
Naoki Ikegami, "Japanese Health Care: Low Cost Through Regulated Fees." Health Affairs, Fall 1991, p.104.
"Dying of Inequality." The Economist. April 4, 1987, p. 52.
Anderson and Rosenberg, "Ontario's Underserviced Area Program Revisited," Table 1, p. 37 and Table 4, p. 39. Statistics are for 1985-86.
Arminee Kazanjian et al.. Fee Practice Medical Expenditures Per Capita and Full-Time Equivalent Physicians in British Columbia. 1987-88 (Vancouver: University of British Columbia, 1989), pp. 121-176.
Ibid.
Kwiko and Rodriguez Neto, "Brazil," The International Handbook of Health Care Systems.
In Brazil, about 75 percent of hospital beds are in private institutions, although the public sector pays for most hospital care. In Venezuela, public sector care is provided only in public hospitals.
Jesus E. Rodriguez and Carlos Sabino, Social Security in Venezuela (Caracas: Cedice). forthcoming.
Joseph Bastien, "Community Health Workers in Bolivia: Adapting to Traditional Roles in the Andean Community," Social Science and Medicine, Vol. 30. No. 3,1990, pp. 281-287.
Kenyon Rainier Stebbins, "Curative Medicine, Preventative Medicine, and Health Status: The Influence of Politics on Health Status," Social Science and Medicine. Vol. 23, No. 2, 1986, pp. 139-148.
See Edmund Wnuk-Lipinski and Raymond Illsley, "International Comparative Analysis: Main Findings and Conclusions." Social Science and Medicine. Vol. 31, No. 8, pp. 879-889.
Ibid., p. 884. See also Elena Mezentseva and Natalia Rimachevskaya, "The Soviet Country Profile: Health of the U.S.S.R. Population in the 70s and 80s: An Approach to a Comprehensive Analysis," Social Science and Medicine, Vol. 31, No. 8, pp. 867877.
Aldona Robbins and Gary Robbins, "What a Canadian-style Health Care System Would Cost U.S. Employers and Employees." National Center for Policy Analysis, NCPA Policy Report No. 145, February 1990.
Ibid.
Ibid.
See Robbins and Robbins, "What a Canadian-style Health Care System Would Cost U.S. Employers and Employees", pp. 2022.
See Uwe Reinhardt, "Health Care Spending and American Competitiveness," Health Affairs, Winter 1989, pp. 5-21.
These and other statistics in this section are taken from Department of Health an Social Security, Health and Personal Social Services for England, 1985 and 1991 editions (London: Her Majesty's Stationery Office, 1985 and 1991).
New charges for these services were introduced in the spring of 1989, however.
See John C. Goodman, "The Envy of the World?", in Arthur Seldon, ed., The Litmus papers: A National Health Disservice(London: Centre for Policy Studies, 1980), pp. 125-132; and Goodman, National Health Care in Great Britain, pp. 192-196.
General Accounting Office, Canadian Health Insurance, p. 38.
Neuschler, Canadian Health Care, p.18.
Michael Walker, "Neighborly Advice on Health Care," Wall Street Journal,June 8, 1988. Cited in Neuschler, Canadian Health Care, p. 51.
See Louise B. Russell, Is Prevention Better Than Cure? (Washington, DC: Brookings Institution, 1986).
Goodman, National Health Care in Great Britain, pp. 55-87.
Ibid., p. 70.
Cooper, Rationing Health Care, p.13.
See Patterns of Prescribing, pp. 21-22.
Elizabeth Rosenthal, "In Canada, A Government System That Provides Health Care to All," New York Times, April 30,1991.
International Journal of Epidemiology, November/December, 1990.
Jon Gabel, Howard Cohen and Steven Fink, "Americans' Views on Health Care: Foolish Inconsistencies?", Health Affairs, Spring 1989, p.111.
Blendon and Taylor, "Views on Health Care: Public Opinion in Three Nations," p.153.
Gabel et al., "Americans' Views on Health Care: Foolish Inconsistencies?", p.110.
Ibid., pp. 109-110.
Ibid., p. 112.
Ibid., p. 114.
See the discussion in Jonsson, "What Can Americans Learn from Europeans?", pp.84-86.
Dr. Gerald L. Musgrave is President of Economics America, a consulting firm in Ann Arbor, Michigan. Dr. Musgrave earned his PH.D. in economics at Michigan State University, and has engaged in teaching and research at California State University, Michigan State University, U.S. Naval Postgraduate School, Stanford University, and the University of Michigan. Dr. Musgrave has written widely on health care and other issues. He is the author or coauthor of over 60 publications. He is the chairman of the Health Economics Roundtable of the National Association of Business Economists and served as a presidential appointee to the National Institutes of Health Recombinant DNA Advisory committee.
He is the chairman of the Academic Advisory Board of the Bahamas Institute of Economic Affairs, and a member of the Advisory Board of the Mackinac Center for Public Policy.
Dr. John C. Goodman is President of the National Center for Policy Analysis in Dallas, Texas. Dr. Goodman earned his Ph.D. in economics at Columbia University and has engaged in teaching and research at six colleges and universities, including Columbia University, Stanford University, Dartmouth College, Sarah Lawrence College and Southern Methodist University. Dr. Goodman has written widely on health care, Social Security, privatization, and other public policy issues. He is author of six books and numerous scholarly articles. His published works include National Health Care in Great Britain, Regulation of Medical Care: Is the Price Too High?, Economics of Public Policy and Social Security in the United Kingdom.
The Mackinac Center for Public Policy is a nonprofit research and educational institute that advances the principles of free markets and limited government. Through our research and education programs, we challenge government overreach and advocate for a free-market approach to public policy that frees people to realize their potential and dreams.
Please consider contributing to our work to advance a freer and more prosperous state.